You run your fingers through your hair in the shower and pause. There's more in the drain than usual. Then you notice the brush filling faster, your ponytail feeling thinner, or your part looking a little wider under bright bathroom light.
That moment can feel upsetting and confusing. The desire for one clear answer, one hormone, one fix is common. In real life, hormone imbalance and hair loss usually don't work that way. Hair thinning is often tied to a hormonal cocktail, not a single lab value. Androgens, estrogen, thyroid hormones, cortisol, and insulin can all shape what your follicles do next.
That complexity can feel overwhelming, but it also gives you a path forward. When you understand which signals are pushing hair out of its normal rhythm, treatment gets more targeted and more realistic. For new parents, that can include postpartum hormone shifts too, and resources like Bornbir support for postpartum parents can help explain why shedding after pregnancy feels so sudden.
Table of Contents
- Is Hormonal Hair Loss Reversible
- How Hormones Regulate Your Hair Growth Cycle
- Which Hormonal Conditions Cause Hair Thinning
- Your Diagnostic Roadmap for Hormonal Hair Loss
- Rebalancing Hormones and Restoring Hair Growth
- Your Integrated Wellness Plan at ProMD Health
- Common Questions About Hormonal Hair Loss
Is Hormonal Hair Loss Reversible
For many people, the first fear is permanent loss. That fear makes sense. Hair is visible, personal, and strongly tied to identity. The encouraging part is that hormonal hair loss is often manageable and sometimes reversible, especially when the cause is identified early and the follicles are still active.
A common example looks like this. Someone in their thirties starts shedding more hair a few months after changing birth control, or during a stressful season with poor sleep and weight changes. Another person enters perimenopause and notices the hairline and part changing at the same time their cycles become irregular. Both may say, “It must be hormones,” and they're often right. But they may be talking about very different hormone patterns.
Why the answer isn't one hormone
Many guides reduce the issue to high androgens alone. That's only part of the picture. Hair follicles respond to a wider set of signals. Current clinical discussion often misses the multifactorial hormonal cocktail where estrogen, DHT, thyroid, cortisol, and insulin interact together, rather than one hormone acting alone, as described in this review of multifactorial hormonal drivers of hair loss.
Hair shedding is often the body's way of saying, “Something changed.” The work is figuring out what changed first.
That's why one person improves when androgen levels are addressed, while another doesn't regrow until thyroid dysfunction, stress load, sleep disruption, or nutrient depletion are corrected too.
What “reversible” really means
Reversible doesn't always mean every strand comes back exactly as it was. It usually means the shedding slows, the growth cycle normalizes, and density improves over time. Some people see stabilization first. That still matters. Stopping ongoing miniaturization or excessive shedding protects what you still have.
In practical terms, the earlier you act, the better your odds of recovery. If you've been waiting for the problem to “just settle down,” it's worth getting a real evaluation instead of guessing.
How Hormones Regulate Your Hair Growth Cycle
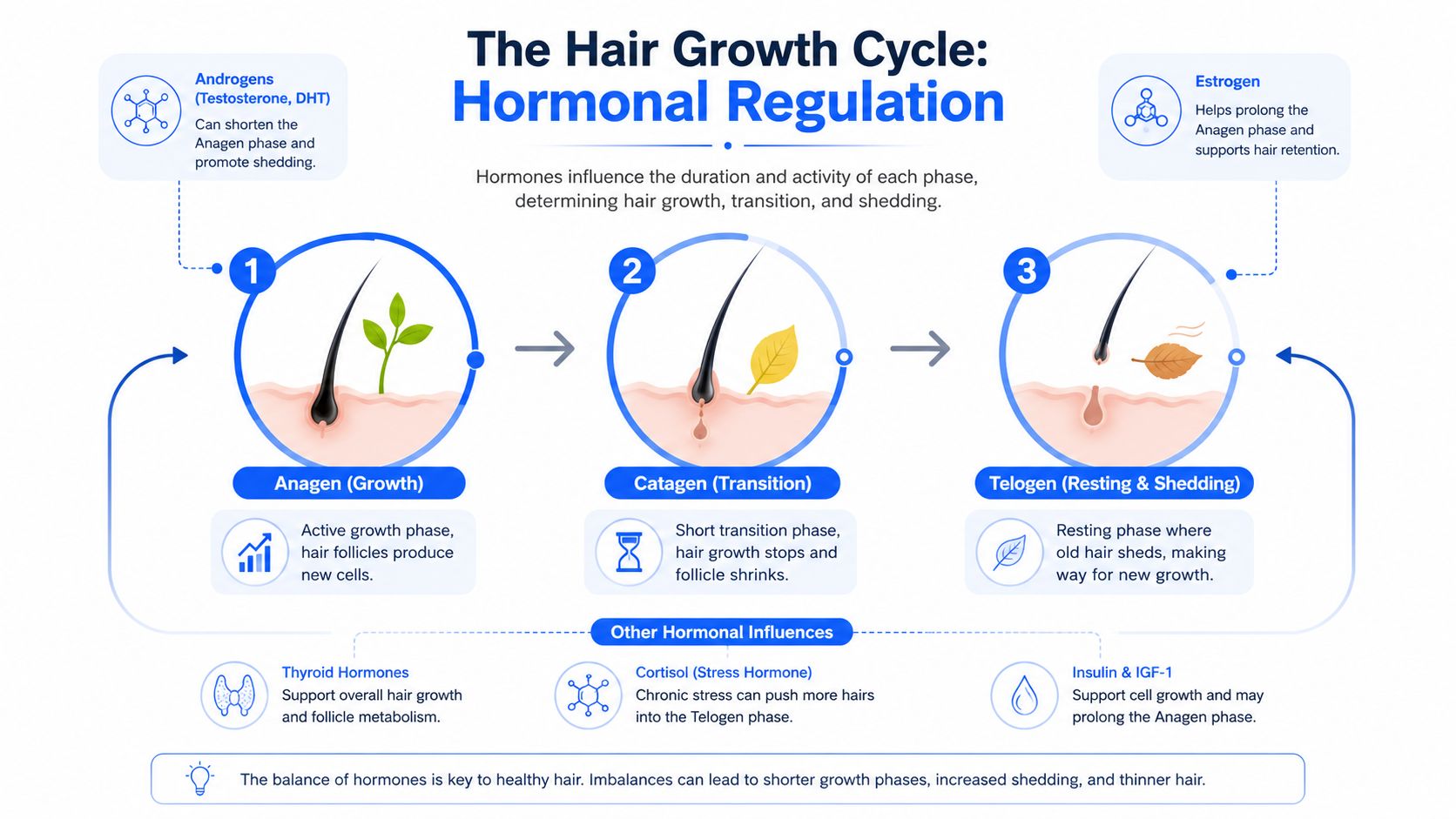
Hair grows in repeating phases, and hormones help set the pace. That timing matters as much as the hair strand itself. A follicle can be present and alive, but if its growth phase is shortened or its resting phase is extended, hair starts to look thinner.
Each follicle moves through three main stages.
- Anagen is the active growth phase. This is when the follicle is building a longer, thicker strand.
- Catagen is a brief transition phase. Growth slows while the follicle resets.
- Telogen is the resting phase. The hair is eventually released so a new cycle can begin.
When this cycle stays on schedule, shedding and regrowth balance each other in the background. You may lose hairs during washing or brushing and never notice a change in density. Problems start when the schedule shifts. Some follicles enter rest too soon. Others do not stay in growth long enough to produce a full-caliber strand.
For readers who want a simple visual explanation of the shaft itself, this stylist's guide to hair structure is a useful companion to understanding what part of the hair you see versus what the follicle is doing under the skin.
How hormones change the timing
Hormones act less like a single on-off switch and more like a group of managers each adjusting one part of the schedule. That is why hair loss often reflects a hormonal cocktail rather than one isolated problem.
Androgens such as DHT can shorten anagen in people with pattern thinning. In plain terms, the follicle gets less time to grow a strong strand before it cycles again. Over many cycles, that can lead to hairs that come in finer, shorter, and easier to miss.
Estrogen helps support a longer growth phase. When estrogen drops, especially during perimenopause or menopause, shedding may become more noticeable and density may slowly decline. This is one reason estrogen deficiency symptoms can show up in the scalp as well as elsewhere in the body.
Other hormones shape the cycle too. Thyroid hormones help keep follicle activity steady. Cortisol can push more hairs into a resting pattern during times of ongoing stress. Insulin affects androgen signaling, which helps explain why blood sugar imbalance and hair thinning can show up together in some people.
A helpful way to picture it is this. The follicle is a tiny factory, and hormones influence the work schedule, supply chain, and maintenance crew at the same time. If one signal is off, the system may compensate. If several signals are off together, growth becomes less reliable.
Here is what that can look like in real life:
- Higher DHT activity may produce progressively finer hairs.
- Lower estrogen support may shorten time spent in active growth.
- Thyroid imbalance may slow the normal rhythm of turnover.
- Chronic stress signals may increase shedding several weeks after the stress began.
- Insulin resistance may amplify androgen-related thinning in susceptible follicles.
Practical rule: Hair loss is not only about how much hair you shed. It is also about whether each follicle gets enough time and the right hormonal support to grow a healthy replacement.
That explains why two people can notice similar shedding in the shower but have very different results over time. One regrows normal strands. The other regrows weaker, smaller hairs because several hormones have changed the follicle's timing at once.
Which Hormonal Conditions Cause Hair Thinning
Those investigating hormone imbalance and hair loss are usually trying to connect their symptoms to a cause. The main categories are easier to understand when you group them by the hormone pattern involved.
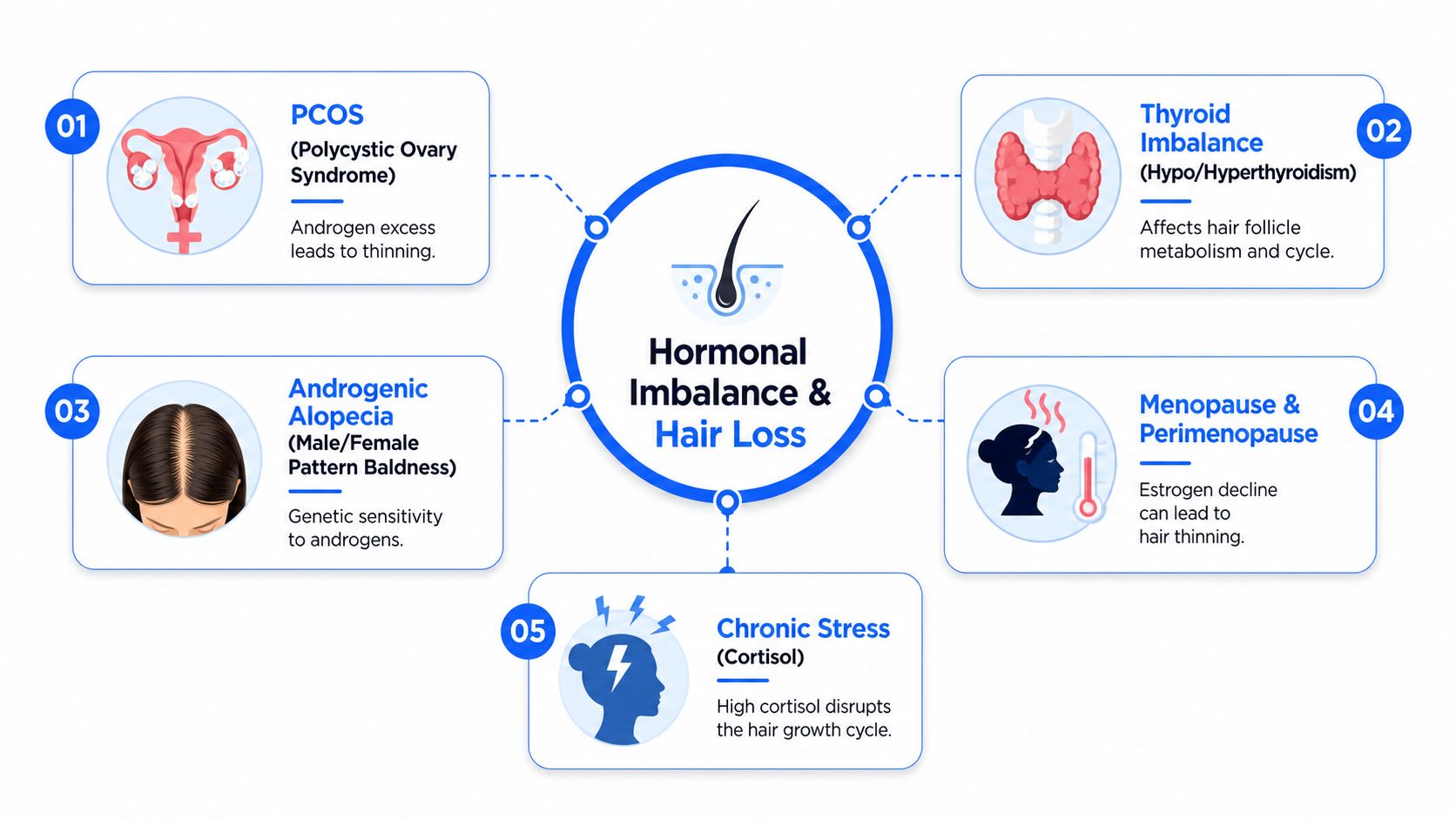
Androgen excess and follicle miniaturization
Androgens are hormones that both women and men make. The issue isn't their existence. The issue is excess levels or increased follicle sensitivity.
PCOS is one of the clearest examples. Hormonal imbalances are major contributors to hair thinning, and in PCOS, androgen excess causes follicle miniaturization, while thyroid disorders are linked to telogen effluvium and alopecia areata, and estrogen deficiency during menopause also leads to hair loss, as outlined in this review of endocrine causes of hair changes.
Miniaturization means the follicle keeps producing hair, but the strand becomes finer, shorter, and less visible with time. That's why some people say, “I'm not going bald in patches, but my hair feels like it's disappearing.”
A clue that androgen excess may be involved is when hair thinning appears along with acne or hirsutism. In women with female pattern hair loss and concurrent hirsutism or acne, treatment with spironolactone shows a 68% better response rate than in women with female pattern hair loss alone, according to this study on androgen-related response patterns in FPHL.
Thyroid shifts and diffuse shedding
Thyroid-related hair loss often looks different. Instead of a widening part alone, people often notice diffuse shedding across the whole scalp.
In thyroid dysfunction, diffuse telogen effluvium affects approximately 50% of individuals with hyperthyroidism and 33% of those with hypothyroidism, with thyroid hormones directly helping regulate the timing of hair cycle transitions, as described in this paper on thyroid hormone effects on the hair follicle.
That matters because thyroid problems can make hair look thinner in a broad, even way rather than in a classic pattern. Hair may also feel drier, more fragile, or slower to recover after shedding.
A second paper reinforces the link, noting that hypothyroidism is a common underlying cause of telogen effluvium and is significantly associated with it in research on hypothyroidism and TE.
Menopause stress and the bigger hormone picture
Menopause and perimenopause often bring thinning that surprises people because it may happen alongside hot flashes, sleep changes, mood shifts, and cycle irregularity. For many, the missing piece is estrogen decline. If that sounds familiar, this overview of estrogen deficiency symptoms can help connect hair changes with other body signals.
Then there's stress. Cortisol doesn't act like DHT or estrogen, but it can still disrupt hair cycling. Insulin patterns can matter too, especially when metabolic symptoms overlap with androgen issues, making the “hormonal cocktail” idea useful. A person may have mild androgen sensitivity, borderline thyroid dysfunction, poor sleep, and chronic stress all at once. No single issue looks dramatic on its own, but together they push follicles into trouble.
If your hair loss story includes stress, cycle changes, skin changes, or energy shifts, that combination often matters more than any one symptom by itself.
Your Diagnostic Roadmap for Hormonal Hair Loss
A good workup should feel organized, not mysterious. The goal isn't to order every test possible. It's to build a clear picture of what your follicles are responding to.
What the first visit should uncover
The first step is a detailed history. A clinician should ask when the shedding started, whether it was sudden or gradual, and what else changed around that time. Useful clues include pregnancy, contraception changes, menopause symptoms, new medications, weight shifts, illness, surgery, stress, scalp symptoms, and family history.
Then comes the scalp exam. That may include looking at the pattern of thinning, checking for miniaturization, examining the hairline, and sometimes doing a gentle pull test to see whether shedding is active. This part helps separate diffuse shedding from patterned loss and from hair breakage.
A practical way to consider this:
- Timeline first. Hair often reacts months after a trigger.
- Pattern second. Diffuse shedding and patterned thinning suggest different mechanisms.
- Whole-body symptoms third. Acne, irregular periods, fatigue, heat intolerance, sleep disruption, and weight changes add context.
What testing often includes
Lab work should answer specific questions. Is the thyroid contributing? Are androgens high? Is estrogen low for the life stage? Are stress, metabolic issues, or nutrient depletion part of the picture?
Testing often includes:
- Thyroid evaluation to look for underactive or overactive patterns.
- Sex hormone review such as testosterone, DHEA-S, or estradiol when symptoms point that way.
- Nutrient checks like iron status or vitamin D when shedding is diffuse or recovery seems slow.
- Metabolic context when insulin resistance or blood sugar instability seems relevant.
Bring a symptom list to your visit. Hair changes make more sense when they're lined up next to cycle patterns, sleep quality, energy, skin changes, and stress load.
The most helpful mindset is this: testing doesn't replace listening to the story. It supports it. Someone can have a “normal” result in one area and still need treatment in another because hair loss rarely follows one simple lane.
Rebalancing Hormones and Restoring Hair Growth
Hair regrowth usually improves when treatment calms the hormone signals affecting the follicle and supports the follicle itself while it recovers. Hair loss from hormone imbalance rarely comes from one switch being flipped. It often reflects a hormonal cocktail. Androgens may be pushing follicles to shrink, estrogen may no longer be buffering that effect, thyroid changes may be slowing growth, cortisol may be keeping more hairs in a resting state, and insulin resistance may be adding fuel to the process.
That is why treatment plans often work best in layers. One layer addresses the hormone pattern. Another supports the scalp and hair cycle. A third removes barriers to recovery, such as nutrient depletion, inflammation, or ongoing physiologic stress.
Treat the root cause and the follicle at the same time
For androgen-related thinning, medications that reduce androgen activity at the follicle can help. Spironolactone is often used in women when symptoms and exam findings suggest androgen excess or androgen sensitivity. Minoxidil remains a common starting treatment because it works directly at the scalp level and can support follicles across several types of hair loss, even while the broader hormone picture is being addressed.
Some patients are also evaluated for finasteride under medical supervision when DHT appears to be a major part of the pattern. The larger point is simple. If the follicle is receiving repeated hormonal signals to miniaturize, scalp treatment alone may not be enough. If the scalp is weak and inactive, hormone treatment alone may also fall short.
Low estrogen can change the picture in a different way. During perimenopause, menopause, or other states of hormone disruption, hair may spend less time in its growth phase and more time shedding. In that setting, a structured hormone plan may be part of treatment. For readers who want a general example of how that care is often organized, this overview of Longevity Medical Institute hormone programs shows how hormone support is commonly framed.
Regenerative care can also have a role, especially when follicles are still present but need stronger growth signaling. A closer look at regenerative medicine for hair loss explains how platelet-rich plasma and related options may fit into a broader medical plan.
A helpful way to picture this is to see the hair follicle as a garden plant. Hormones shape the season, the scalp is the soil, and treatment works best when both are improved. Watering a plant in poor soil has limits. Fixing the soil without enough water has limits too.
Comparing Hair Restoration Treatments
| Treatment | How It Works | Best For | ProMD Health Approach |
|---|---|---|---|
| Minoxidil | Supports follicles at the scalp and encourages growth activity | Many forms of thinning, especially as a starting therapy | Often used as a foundation while the underlying cause is investigated |
| Spironolactone | Reduces androgen effect on the follicle | Female pattern hair loss with signs of androgen involvement | Considered when symptoms suggest androgen excess or sensitivity |
| Finasteride | Lowers DHT activity | Selected androgen-driven cases under medical guidance | May be included when DHT appears central to the pattern |
| Hormone optimization | Addresses broader hormone imbalance such as menopausal change | Hair loss tied to low estrogen or wider endocrine symptoms | Integrated with symptom review, labs, and follow-up |
| PRP | Uses platelet-rich plasma to stimulate follicles | People who want a non-surgical regenerative option | Combined with medical treatment when appropriate |
| Nutrition and lifestyle support | Corrects gaps that interfere with recovery | Diffuse shedding, stress-related patterns, low iron or low resilience | Paired with medical treatment rather than treated as an afterthought |
The right plan depends on the pattern of loss and the hormone mix behind it. A person with stress-related shedding after a hormone shift needs a different strategy than someone with long-standing follicle miniaturization driven by androgen sensitivity. That distinction matters because restoring hair growth is rarely about one hormone in isolation. It is about improving the whole signaling environment the follicle lives in.
Your Integrated Wellness Plan at ProMD Health
Hair loss tied to hormones often frustrates people because they get fragmented care. One visit focuses on the scalp. Another focuses on menopause. Another focuses on stress or weight change. The pieces don't always get connected.

Why coordinated care matters
An integrated model works better for hormone imbalance and hair loss because follicles respond to whole-body signals. If thyroid patterns, menopause symptoms, stress load, nutrient issues, and androgen sensitivity are all active, isolated treatment usually falls short.
That's where a coordinated plan becomes practical. ProMD Health offers hormone optimization, menopause management, hair loss care, and regenerative options within the same broader medical framework, with telehealth support through ProMD Connect for ongoing management in its service areas. That matters when someone needs follow-up, prescription oversight, symptom tracking, and treatment adjustments rather than a one-time recommendation.
Good hair treatment often looks like good systems care. The scalp improves when the body's signals become more stable.
What an integrated plan can include
A realistic wellness plan may combine several layers:
- Medical evaluation for thyroid, androgen, estrogen, or metabolic patterns
- Hormone support when symptoms and labs point that way
- Hair-focused therapy such as topical treatment or regenerative options
- Lifestyle correction for stress, sleep, and nutrient intake
- Remote follow-up so treatment can be adjusted as your body changes
The cash-pay model is also worth understanding clearly. It means care isn't framed around insurance approval rules. Instead, plans can be built around clinical judgment, available services, and ongoing monitoring. For many people dealing with complex hormone symptoms, that allows for more personalized decision-making.
Common Questions About Hormonal Hair Loss
Can hormonal hair loss grow back
Yes, it can, especially if the trigger is identified and addressed while follicles are still active. Some people regain density. Others first notice that shedding slows and the hair they keep becomes stronger. That still counts as progress.
How long does treatment take to work
Hair is slow tissue. Even the right plan takes patience because follicles need time to move through their cycle. Individuals can expect change in phases: less shedding first, then early regrowth, then gradual improvement in density and texture.
Can birth control cause or help hair loss
Both are possible. Hormonal contraception can trigger shedding in some people, especially after starting, stopping, or switching formulations. Verified data also note that surveys involving thousands of female patients found 8 out of 10 women under 40 attributed their hair loss to hormonal contraception use or hormonal changes in the review of endocrine hair disorders cited earlier. At the same time, some formulations may help when androgen excess is part of the problem. This is one reason individualized evaluation matters. You can also learn more in these common questions about a hormonal imbalance.
Are supplements enough on their own
Sometimes they help, but they usually aren't enough if the main driver is androgen excess, thyroid dysfunction, menopause, or another active hormonal issue. Supplements support recovery best when they fill a real gap inside a broader treatment plan.
If you're noticing shedding, widening at the part, or hair that no longer feels like your own, ProMD Health offers medically supervised support for hormone optimization, menopause management, and hair restoration so you can investigate the cause and build a plan that fits your symptoms.