You may be in a familiar place right now. You've cleaned up your diet, started over on Monday more times than you can count, lost some weight, then watched it return when life got busy, hormones shifted, stress climbed, or hunger became too hard to fight.
That cycle is exhausting because it makes a complex medical issue feel like a personal failure. In reality, weight gain and weight regain often involve appetite signaling, insulin response, medications, sleep, stress, hormone changes, and body composition changes that a generic diet can't fully address. A clinical process can help when self-directed efforts haven't held up.
Table of Contents
- Beyond the Scale a New Approach to Lasting Weight Loss
- What Medically Supervised Weight Loss Really Means
- The Clinical Components of a Weight Management Program
- Who Is an Ideal Candidate for This Approach
- Timeline Expectations and Sustainable Outcomes
- The ProMD Health Difference Integrating Wellness and Aesthetics
- Frequently Asked Questions About Medical Weight Loss
Beyond the Scale a New Approach to Lasting Weight Loss
Most diets ask you to do one thing. Eat less and try harder. That advice ignores why your body may be resisting change in the first place.
Medically supervised weight loss is different because it starts with evaluation, not blame. Instead of assuming every patient needs the same calorie target or the same meal template, a medical team looks at what may be driving weight gain or blocking progress. That can include metabolic factors, medication side effects, hormone shifts, poor sleep, stress, low muscle mass, or a pattern of losing and regaining weight repeatedly.
A structured program also changes the way progress is measured. The goal isn't only a lower number on the scale. The goal is safer fat loss, preservation of health, improved function, and a plan you can continue when motivation fluctuates.
Practical rule: If your past attempts worked only while you were white-knuckling them, the issue often isn't effort. It's that the plan wasn't built for your physiology.
This kind of care is especially helpful for people who want more than a short burst of results. It gives you regular follow-up, course correction, and medical context when the process gets harder. That's often the missing piece.
If you're early in the process and want a clear overview of how treatment begins, this weight management starting guide is a useful next step.
A good program also removes some of the confusion. You don't have to guess whether your plateau means the plan failed, whether medication is appropriate, or whether your symptoms point to a larger issue. Those questions should be handled clinically.
Here's what this approach usually changes in practical terms:
- Assessment replaces guessing: Your history, current health, and patterns matter.
- Treatment becomes personalized: Nutrition, activity, supplements, and medication are selected based on your needs.
- Follow-up becomes part of success: Adjustments happen before frustration turns into quitting.
That shift matters because long-term weight change rarely comes from intensity alone. It comes from a plan that your body can respond to and a care team that can adapt it over time.
What Medically Supervised Weight Loss Really Means
A lot of people hear the term and assume it means a quick prescription and a few generic instructions. That isn't what careful treatment looks like.
Clinical oversight changes the starting point
The word supervised matters. A medical provider reviews your health history, current medications, symptoms, prior attempts, and treatment goals. Follow-up visits then track how you're responding, whether side effects are emerging, and whether the plan should change.
That level of oversight isn't cosmetic. In a medically supervised intervention for high-risk obesity, patients who completed at least six visits achieved a mean weight loss of 7.06% from their initial program start date, with about 50% exceeding 7% total weight loss and more than 55% achieving at least 3% weight loss regardless of BMI classification, according to a specialized medical weight management study. The same report found that those with six or more months of visit activity had better average weight loss than those with only four to five months of activity.
In other words, supervision isn't just about safety. It also supports consistency and better decision-making over time.
A plan should fit your biology, not the other way around
The word medical matters just as much. A real program doesn't force every patient into the same template. It builds a health blueprint around the person in front of you.
That often includes a mix of elements such as:
- Nutrition guidance: Enough structure to create progress, without turning every meal into a test of willpower.
- Behavioral support: Patterns around hunger, routine, stress eating, travel, and weekends need strategies, not shame.
- Evidence-based tools: Some patients do well with lifestyle support alone. Others benefit from prescription therapy, supplements, or additional metabolic evaluation.
Medical weight loss works best when the treatment matches the reason you're struggling.
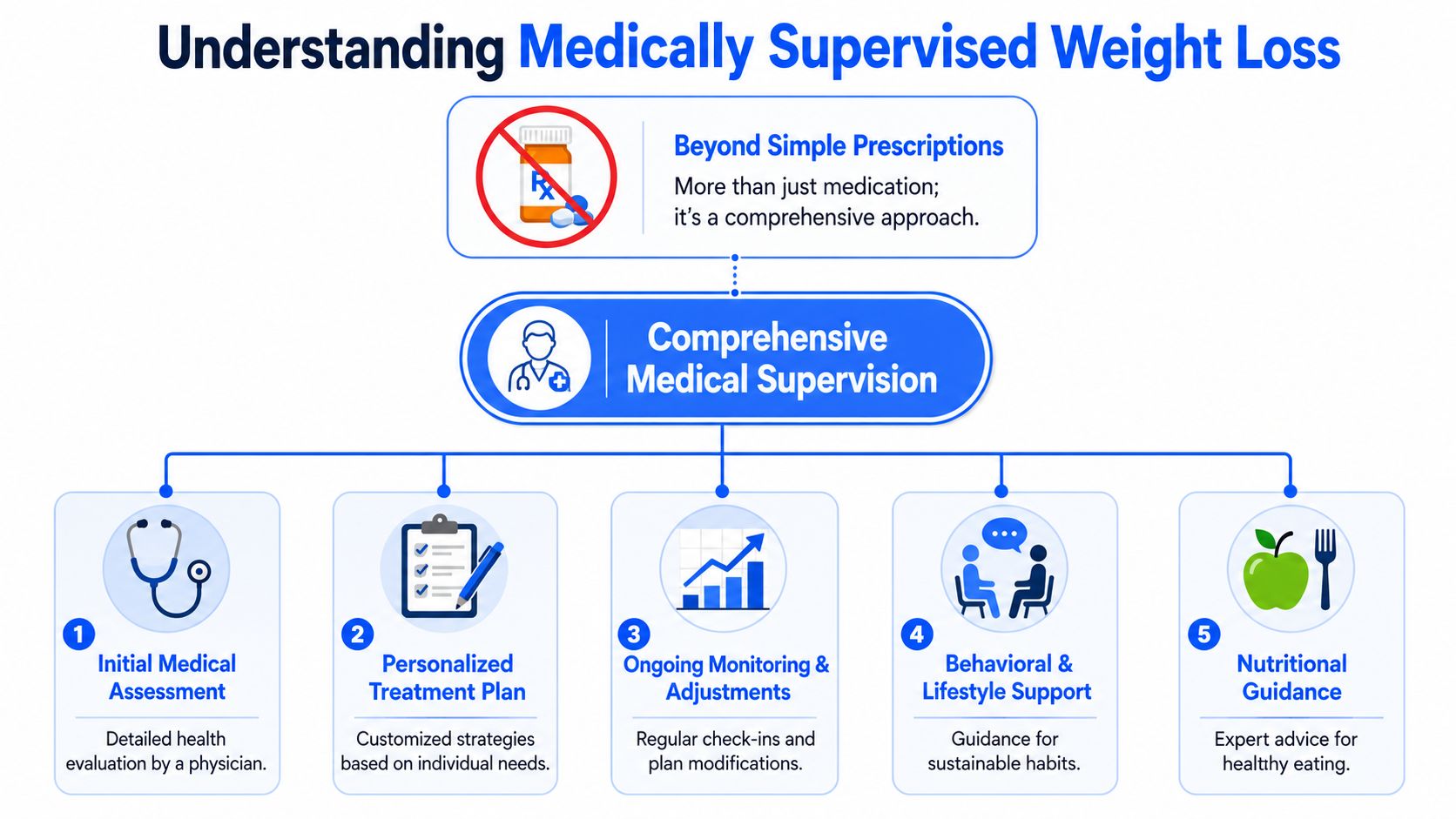
There's another important point patients often appreciate hearing clearly. Prescription medication can be part of treatment, but it isn't the definition of treatment. The strongest programs combine medical judgment, follow-up, and sustainable lifestyle work so that every tool has a purpose.
The Clinical Components of a Weight Management Program
Once people understand the concept, the next question is usually practical. What happens in the program?

Medication is one tool, not the whole program
For some patients, prescription therapy can make treatment more effective by addressing appetite regulation and energy balance. Systematic reviews of clinical trials found that combining reduced-energy diets with pharmacotherapy produced a mean weight loss of 5 to 8.5 kg, or about 5% to 9%, during the first six months, with sustained loss of 3% to 6% maintained up to 48 months in many cases, based on this systematic review on long-term weight-loss maintenance.
Specific GLP-1 treatment data is also meaningful. In multi-center clinical trials, patients receiving GLP-1 receptor agonists under medical supervision achieved a mean reduction of 14.9% of initial body weight at 68 weeks, and 87% lost at least 5% of their starting weight, according to clinical trial data referenced by ProMD Health.
That doesn't mean everyone needs medication. It means medication can be appropriate when hunger, cravings, insulin response, or prior treatment failure suggest that lifestyle support alone may not be enough.
For patients using these therapies, meal structure matters. Practical support like meal planning for GLP-1 users can help patients eat consistently, protect protein intake, and avoid the under-eating or nausea-related patterns that sometimes derail progress.
A deeper look at how these medications fit into metabolic care is available in this overview of GLP-1 medications and metabolic health.
Habits, monitoring, and adjustments drive the long game
Medication doesn't replace the rest of the program. It creates room for better adherence when used correctly. The clinical framework still relies on several moving parts working together.
| Component | Why it matters |
|---|---|
| Nutrition counseling | Helps create an eating pattern you can repeat without extremes |
| Exercise prescription | Supports muscle retention, function, and metabolic health |
| Behavioral strategies | Addresses triggers, routines, and decision points that affect eating |
| Medical monitoring | Tracks tolerance, progress, symptoms, and needed adjustments |
A do-it-yourself plan usually misses two things. First, it rarely identifies why progress stalls. Second, it doesn't adapt quickly when the original plan stops working.
Group care can also matter in some settings. Data comparing group medical visits with individual visits found average losses of 11.63 lbs in group visits versus 3.99 lbs in individual visits, along with stronger retention and more patients achieving greater than 7% weight loss, based on this study of group medical visits for weight management. That finding reinforces a practical truth. Support structure changes outcomes.
Who Is an Ideal Candidate for This Approach
Not everyone needs a medical program. Some people respond well to straightforward nutrition changes and a consistent exercise routine. Others need a higher level of structure because their situation is more complicated than a standard diet can solve.
Good candidates usually share a pattern
This approach is often a strong fit for adults who see themselves in one or more of these situations:
- Repeated weight regain: You can lose weight, but you can't maintain it once the plan becomes harder to sustain.
- Weight-related health concerns: Your weight is affecting blood sugar, blood pressure, mobility, sleep, or day-to-day energy.
- Complex biology: Menopause, hormone changes, medication-related gain, appetite dysregulation, or metabolic resistance may be part of the picture.
- Need for accountability: You know what to do in theory, but consistency improves when someone is reviewing your progress and adjusting the plan.
Some patients also come in with a very specific concern area rather than a broad weight-loss goal. Midsection changes around perimenopause and menopause are common examples. For a practical patient-friendly read on that issue, strategies for women's midsection weight can help explain why the problem often feels different in this phase of life.
Readiness matters as much as the number on the scale
A good candidate doesn't have to be perfect. You don't need flawless eating habits or a perfect gym routine before seeking help. But you do need a willingness to participate sincerely in a structured process.
That usually means being ready to:
- Attend follow-up visits: Progress is built through review and adjustment.
- Track patterns: Hunger, side effects, sleep, stress, and adherence all matter.
- Accept gradual change: Sustainable treatment isn't the same as a crash diet.
- Work on more than food: Sleep, movement, hormones, and routine often need attention too.
The best candidates aren't the most disciplined people in the room. They're the ones ready to stop improvising and start treating weight as a health issue that deserves proper care.
Timeline Expectations and Sustainable Outcomes
People often want one answer to the question, “How long will this take?” Realistically, the journey has phases. What matters most is that each phase has a purpose.

The first phase is assessment and momentum
The process usually begins with consultation, medical review, and diagnostic work that clarifies what treatment should look like. That early stage can feel slower than a commercial diet, but it's often where the most important decisions are made. A rushed start can produce the wrong plan.
From there, active treatment builds. Medically supervised programs that include clinical guidance, prescription medications, and nutritional supplements produce an average 10% to 15% total body weight loss over 6 to 12 months, while lifestyle-only interventions typically yield 2% to 5%, according to data on medically supervised weight management outcomes.
Those numbers matter because even moderate weight reduction can change how patients feel physically. Breathing, movement, hunger control, and confidence often improve before the final goal weight is reached.
A plateau is also normal. It doesn't mean your body is “broken,” and it doesn't mean the plan failed. It means your body has adapted and the plan may need recalibration. That's one reason regular follow-up is so useful.
Maintenance is part of treatment, not an afterthought
The most overlooked phase is what happens after early momentum. Patients often assume maintenance begins when motivation is high and the hard part is over. In reality, maintenance starts while treatment is still active.
Long-term data supports that approach. In a medically supervised program built around an initial four-month meal replacement phase, weekly behavioral intervention, and medical monitoring, average weight loss reached 15.3% after four months. At the five-year follow-up, average weight loss remained -5.8%, and about 50% of participants maintained at least 5% total weight loss, based on this long-term medically supervised weight management study.
That kind of result doesn't happen because patients stay in a perfect fat-loss phase forever. It happens because the program teaches transition, recovery after setbacks, and long-range habit building. If you're working on the behavioral side of maintenance, resources that help develop lasting weight loss habits can support the day-to-day side of consistency.
The ProMD Health Difference Integrating Wellness and Aesthetics
Weight care is most useful when it doesn't stop at the prescription pad or the scale. Many patients want better metabolic health, but they also want to feel stronger, more confident in their shape, and more like themselves again.
Weight care works better when root causes are addressed
An integrated model matters because weight change often overlaps with hormone health, sleep quality, inflammation, body composition, and aging-related concerns. Some people need appetite treatment. Others need a closer look at menopause symptoms, medication-related gain, or low-energy patterns that make exercise harder to sustain.
ProMD Health offers medically supervised weight management through an integrated care model that combines clinical evaluation, prescription therapy, and supplement support, and it operates across 17 approved locations, including Annapolis, MD, Arlington, VA, and Washington, DC, as listed on the ProMD Health locations page.
For patients considering care, the weight management service page outlines how clinical guidance, prescriptions, and ongoing support fit together.
Body confidence often needs more than a lower scale number
A comprehensive model is particularly beneficial, as significant weight loss can improve health while still leaving patients with concerns about muscle tone, body contour, or stubborn areas that don't respond the way they expected.
An integrated clinic can address those next-step concerns more realistically. If a patient loses weight but wants better muscle definition, body contouring support may become relevant. If hormone shifts are contributing to fatigue and central weight gain, hormone optimization may improve the overall treatment picture. If the goal is long-term wellness, remote follow-up through telehealth can help maintain continuity when in-office visits aren't practical.
Better weight care isn't only about getting lighter. It's about helping your health, shape, energy, and confidence make sense together.
That broader lens is often what turns short-term success into something that feels sustainable.
Frequently Asked Questions About Medical Weight Loss
Is medical weight loss covered by insurance
At ProMD Health, weight management services are offered on a cash-pay model, so they aren't covered by insurance. That's important to state clearly because many patients assume a medical program automatically works like a traditional insurance-based office visit.
The right next step is to ask for current program details directly so you understand what is and isn't included. A transparent plan should explain visits, monitoring, prescriptions if appropriate, and any supplements or related services before you begin.
Do I have to take prescription medication
No. Medication can be helpful, but it isn't required for every patient. Many patients achieve excellent results with nutrition guidance, exercise, behavioral coaching, and metabolic testing alone, especially when root causes like medication-induced weight gain or hormonal imbalances are addressed without drugs, as discussed in this medical supervision overview from Core Primary Care.
That matters because some patients want a medication-free plan, while others need medication as one part of a broader strategy. Good care makes that decision case by case.
What side effects can happen with weight loss medications
Side effects depend on the medication being used. In practice, the most common issues patients ask about are digestive changes, appetite shifts, nausea, constipation, or feeling overly full. Those effects are one reason medical follow-up matters.
A careful program manages side effects by adjusting dose timing, food choices, hydration, pacing, and the treatment plan itself when needed. If a medication isn't a good fit, the answer isn't to push through blindly. The answer is to reassess.
What if I've failed other programs before
That's more common than is commonly recognized, and it doesn't mean you're a poor candidate. It usually means the prior plan wasn't specific enough, wasn't medically informed, or wasn't sustainable in real life.
The strongest next step is to review what happened in detail. Did hunger win out? Did life disruptions break the routine? Did the weight come back after you stopped a rigid plan? Those answers help shape a better one. Previous failure is often useful clinical information.
If you're ready to explore a more structured, medical approach to weight management, ProMD Health offers consultations focused on identifying root causes, selecting appropriate treatment options, and building a plan that supports both health and long-term confidence.


