Those asking about regenerative medicine are really asking the wrong question. They ask, “What treatment is newest?” when the better question is, “Which therapies improve tissue quality, which only create a temporary effect, and how do they fit into a bigger plan for aging well?”
That distinction matters. Fillers, neurotoxins, peels, and lasers still have an important place, but they don't all work the same way. Some camouflage loss. Some stimulate repair. A few do both. Regenerative medicine examples sit in that second category. They try to improve the environment inside the tissue so skin, hair, connective tissue, and even systemic recovery can perform better over time.
This isn't fringe medicine anymore. One market analysis estimated regenerative medicine at USD 34.6 billion in 2022 and projected USD 194.9 billion by 2032, a 19.4% CAGR, while another forecast placed the market at USD 58.40 billion in 2026 and USD 360.84 billion by 2034, a 25.56% CAGR. A separate U.S. report valued the market at USD 16.81 billion in 2023 and projected a 16.72% CAGR through 2030, according to regenerative medicine market statistics. That tells you the category has moved well beyond a lab concept.
In aesthetics and wellness, true value is strategic use. The best results rarely come from one “miracle” procedure. They come from matching the right regenerative tool to the right problem, then combining it with hormonal health, skin maintenance, energy-based devices, and realistic timelines. That's where patients usually get misled. They hear broad promises, but not enough about maturity, evidence, access, safety, or what is routine versus still emerging.
Table of Contents
- 1. Platelet-Rich Plasma (PRP) Therapy
- 2. Adipose-Derived Stem Cell Grafting (ADSCG) and Stromal Vascular Fraction (SVF)
- 3. Biostimulatory Collagen Induction with Sculptra
- 4. Laser-Assisted Tissue Regeneration (Multiple Modalities)
- 5. Microneedling and Radiofrequency Microneedling
- 6. Peptide Therapy and Growth Factor Supplementation
- 7. Exosome Therapy and Extracellular Vesicle Technology
- 8. Emsculpt NEO and Electromagnetic Muscle Stimulation
- 9. Hair Restoration with Low-Level Laser Therapy (LLLT) and Combination Protocols
- 10. Hormone Optimization and Regenerative Endocrinology
- 10-Item Regenerative Medicine Comparison
- Choosing Your Partner in Regeneration
1. Platelet-Rich Plasma (PRP) Therapy
PRP remains one of the most practical regenerative medicine examples because it's simple, autologous, and versatile. A sample of your blood is processed, the platelet-rich fraction is isolated, and that concentrate is placed back into tissue where you want a repair signal. In skin, that usually means collagen support and texture improvement. In scalp work, it means creating a better environment around weakened follicles.
What I like about PRP is that it's biologically conservative. You're not introducing a synthetic filler or a foreign biologic. You're using your own blood components to stimulate repair. That makes it attractive for patients who want a lower-intervention starting point for facial rejuvenation or hair restoration.
Why PRP still earns a place
The trade-off is speed. PRP doesn't create an instant visible correction the way hyaluronic acid filler does. It asks for patience, repeat sessions, and realistic expectations. It's often best for early tissue decline, post-procedure recovery support, fine textural change, or as part of a multi-step hair protocol.
- Best use case: Early thinning hair, dull skin quality, crepey under-eye texture, and support after microneedling.
- Main limitation: Results are operator-dependent and patient-dependent. Platelet quality varies.
- Who should pause: Patients on blood thinners, people who hate blood draws, and anyone expecting dramatic next-week results.
Practical rule: PRP works best when the tissue is stressed, not destroyed. It's a support therapy, not a replacement for surgery or deep structural correction.
For patients considering scalp treatment, it helps to understand the process and expectations before starting. ProMD Health's guide on explaining PRP treatments gives a useful overview, and this outside primer offers additional details on PRP treatment.
2. Adipose-Derived Stem Cell Grafting (ADSCG) and Stromal Vascular Fraction (SVF)
If PRP is a signaling treatment, fat-based regenerative grafting is a structural and biologic treatment at the same time. That's why ADSCG and SVF stand apart from many other regenerative medicine examples in aesthetic practice. You aren't just asking tissue to behave younger. You're also restoring volume with living material from the patient.
In practical terms, a small amount of fat is harvested, processed, and reinjected where facial or body tissue has thinned. The value isn't just the volume. It's the regenerative cell population and tissue-supporting matrix that come with it. For the right patient, that can create a softer, more integrated result than repeating filler year after year.
Where fat-based regeneration outperforms filler
This is the better choice when someone has true volume loss, poor skin quality, and a desire for a more biologic correction. It's especially useful in faces that look depleted rather than wrinkled. Patients who've become overfilled with conventional filler can also do well when the plan shifts toward restoration instead of repeated product stacking.
The downside is commitment. There's harvesting, processing, reinjection, recovery, and the need for technical expertise. Some of the transferred volume won't persist exactly as placed, so planning matters.
- Strong candidate: Lean or aging faces with hollow temples, midface loss, lower-face deflation, or a history of poor filler longevity.
- Less ideal candidate: Someone who wants a lunch-break treatment with no recovery.
- Clinical advantage: It treats contour and tissue quality together, which is hard to achieve with a single syringe-based solution.
In an integrated practice, this kind of treatment usually works best when paired with skin-based therapies afterward. The graft restores the scaffold. Then lasers, biostimulators, skincare, and hormone optimization support how that scaffold ages.
3. Biostimulatory Collagen Induction with Sculptra
What do you do when a face looks thinner, less supported, and less resilient, but adding more filler would push it in the wrong direction?
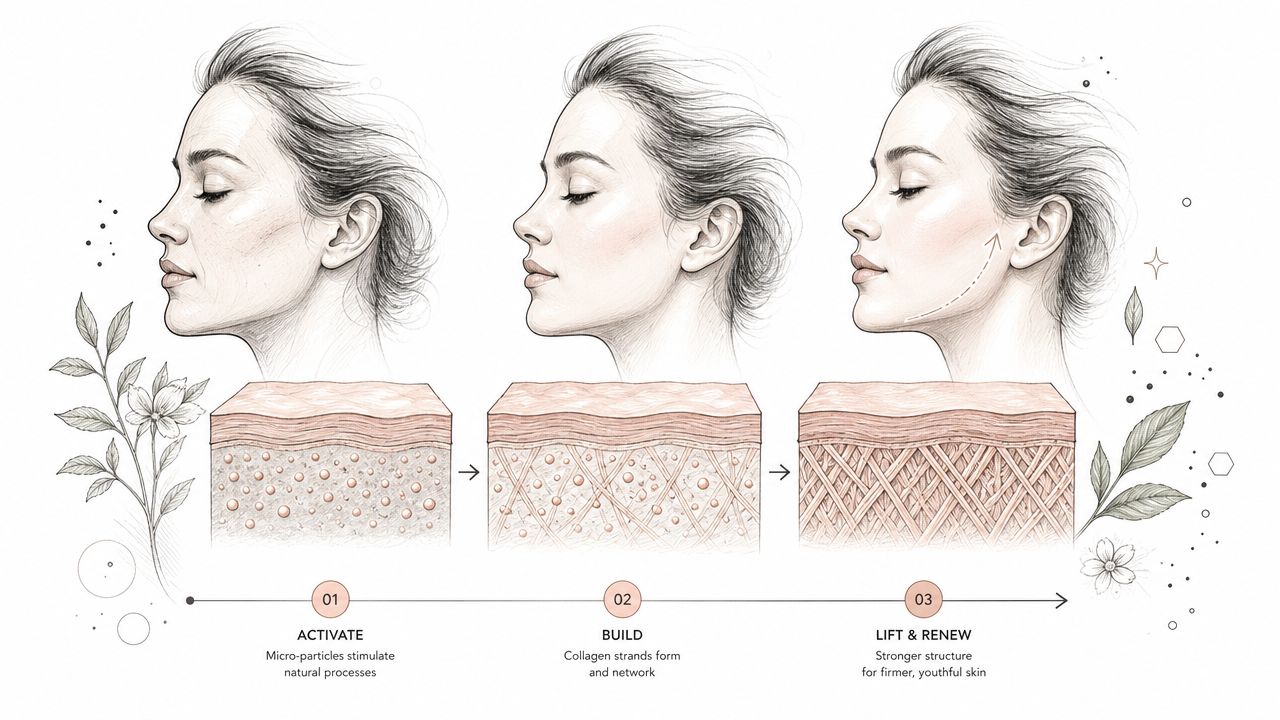
Sculptra often fits that problem well. It earns a place in regenerative medicine examples because the goal is collagen induction through a biostimulatory injectable, not simple space-filling. In practice, that makes it useful for patients who need gradual structural improvement and better tissue support rather than a quick increase in volume.
That distinction matters in mature faces and in patients who already have product in the tissue. Sculptra can improve firmness, contour support, and skin quality over time when it is diluted properly, placed at the correct depth, and mapped to the patient's pattern of volume loss. The result is usually subtler at first and more convincing months later.
A simple visual helps explain the process:
The right patient for Sculptra
The best candidates are patients with diffuse facial thinning, early jowling, temple hollowing, cheek flattening, or lower-face laxity who want a more biologic correction. Sculptra also works well for patients who say they look tired or deflated, but do not want a filled or sharply contoured look. In an aesthetic and wellness practice, I view it as a tissue-quality treatment with shaping benefits, not as a one-visit substitute for every volume problem.
Trade-offs need to be clear. Results build slowly. Most patients need a treatment series, and the final outcome depends on collagen response, treatment spacing, and injector technique. It is a poor fit for someone who wants immediate correction before an event, and it is not the product I reach for when a patient needs crisp definition in a very specific area.
Technique and aftercare matter. Poor placement, overcorrection, or weak patient selection can produce an uneven result or disappointment because the timeline was misunderstood. Sculptra rewards planning, patience, and a full-face strategy.
For patients comparing options, ProMD Health outlines the treatment approach in this discussion of Sculptra for facial lifting and collagen support.
Within a broader regenerative plan, Sculptra often works best as one layer of treatment rather than the whole answer. I commonly place it alongside skincare, energy-based treatments, hormone optimization when indicated, and other interventions that support how the collagen matrix ages after injection. That is where it becomes more than a cosmetic injectable. It becomes part of a longer-term restoration strategy.
4. Laser-Assisted Tissue Regeneration (Multiple Modalities)
Lasers deserve a place on this list because controlled injury is still one of the most reliable ways to trigger dermal remodeling. Whether the device is ablative, non-ablative, or fractional, the principle is similar. You create a measured wound or heat response, and the skin begins a repair cascade.
That doesn't mean every laser is “regenerative” in the same way. Some remove damaged surface layers very effectively but come with more downtime. Others heat deeper tissue with less disruption but also more modest change per session. The mistake patients make is treating all laser work as one category.
Matching the modality to the problem
For rough texture, etched lines, acne scarring, and sun-damaged skin, ablative or fractional resurfacing often has the strongest role. For collagen support with less downtime, non-ablative options can make more sense. For redness, vessels, or pigment, wavelength selection matters more than raw intensity.
The best outcomes happen when lasers are sequenced properly within a broader plan.
- Use lasers for: Texture, pigment, vascular irregularity, pores, scars, and resurfacing.
- Don't use lasers alone for: Major facial deflation, hormonal hair loss, or systemic aging symptoms.
- Expect this trade-off: The more aggressive the improvement goal, the more healing discipline you'll need afterward.
Laser patients also need honesty about risk. Post-inflammatory hyperpigmentation, prolonged redness, acne flares, and barrier disruption are real concerns if skin type, settings, and aftercare are handled poorly. In a wellness-oriented practice, that's why pretreatment skin conditioning and post-laser recovery support matter almost as much as the laser itself.
5. Microneedling and Radiofrequency Microneedling
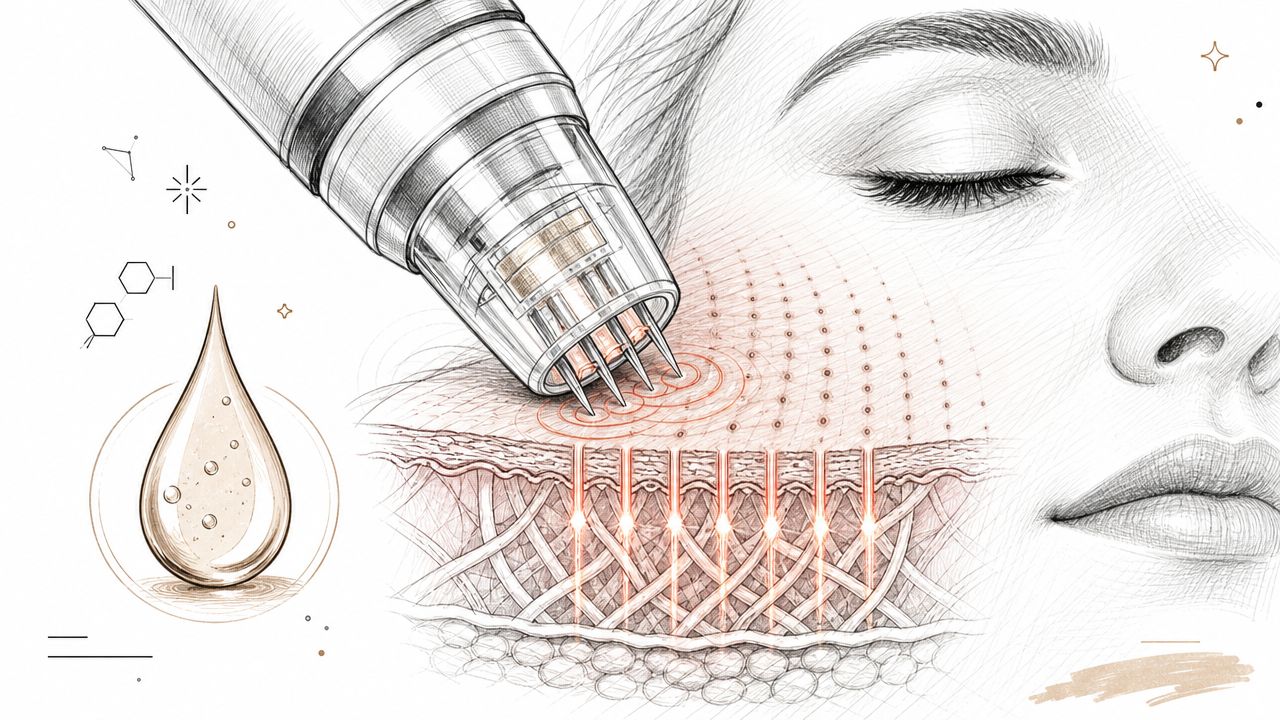
Not every regenerative treatment has to be dramatic to be useful. Microneedling and radiofrequency microneedling are workhorse options because they improve tissue quality with a much lower barrier to entry than more aggressive resurfacing. They create controlled micro-injury, which stimulates collagen remodeling. RF microneedling adds thermal energy deeper in the dermis, which can strengthen the response in laxity and acne-scar patients.
In real practice, these devices are often better for consistency than spectacle. They're not usually the treatment that changes a face overnight. They are the treatment that keeps skin improving steadily when repeated on a good schedule.
Here's the basic concept visually:
Where microneedling wins
If you have acne scarring, enlarged pores, early skin laxity, or crepey texture, microneedling often belongs in the plan. If you have severe sun damage or prominently etched wrinkles, it may be a useful support treatment but not the primary one.
I often think of standard microneedling as the flexible option and RF microneedling as the more corrective option.
- Standard microneedling: Better for texture support, maintenance, and combination with PRP or topical recovery products.
- RF microneedling: Better when scars, skin tightening, or deeper remodeling are priorities.
- What doesn't work: Sporadic sessions with no skincare, no sun discipline, and no maintenance strategy.
The patients who say microneedling “did nothing” often had the wrong target, the wrong depth, or too few sessions.
This category also integrates well with regenerative protocols because it creates channels and biologic signaling that can complement PRP and other recovery-focused strategies.
6. Peptide Therapy and Growth Factor Supplementation
Peptides attract a lot of attention because they sit at the intersection of aesthetics, recovery, performance, and longevity. In an integrated practice, they can make sense when the goal isn't just a prettier surface but better healing capacity, support during weight loss, improved recovery, or adjunctive help in hair and skin programs.
The problem is that this category is uneven. Some peptide discussions are thoughtful and medically supervised. Others are driven by hype, loose sourcing, and very casual promises. That's why I treat peptides as supporting tools, not as standalone answers.
Useful, but only with good clinical judgment
Peptide therapy may fit patients who are already working on several fronts at once. For example, someone in a medically supervised weight program who is also addressing hair thinning, poor sleep, slow recovery, or inflammatory skin changes may benefit from a broader systems-based approach. In that setting, peptides can be part of the conversation.
Their role is usually supportive rather than visibly making fundamental changes on their own.
- Potential fit: Recovery support, wellness optimization, hair and skin adjunct protocols, and patients already engaged in broader medical care.
- Main caution: Product quality and regulatory status vary. Oversight matters.
- Wrong expectation: Thinking a peptide protocol will replace procedures, nutrition, hormone correction, or evidence-based hair-loss management.
For patients exploring that side of care, this overview on how to support wellness with peptide therapy gives a general consumer-oriented introduction. The important clinical point is that peptide use should sit inside a real treatment plan, not outside one.
7. Exosome Therapy and Extracellular Vesicle Technology
What are exosomes doing in a regenerative treatment plan, and where do they fit better than more established options?
Exosomes and other extracellular vesicles are attracting attention because they target signaling rather than cell transplantation. The clinical idea is straightforward. Instead of placing living cells, the goal is to deliver biologically active messengers that may influence inflammation, repair behavior, and tissue response.
That makes the category interesting. It also makes patient selection, product selection, and expectation-setting more important than the marketing usually suggests.
A conceptual image helps explain the basic mechanism patients are reacting to with this technology:
A signaling tool with real limitations
In aesthetic practice, exosome-based products are usually discussed for skin quality, post-procedure recovery support, and hair restoration protocols. Those are reasonable areas of interest because tissue regeneration depends heavily on cell-to-cell communication. But exosomes are not a magic shortcut to better outcomes. Results depend on source material, processing standards, storage conditions, delivery method, and whether the indication makes biological sense in the first place.
That is the practical trade-off. The science is promising, but the category is less settled than PRP, collagen stimulators, energy-based devices, or well-built combination hair programs.
I treat exosomes as an adjunct, not a default starting point. In a real clinic, they may have value after microneedling, laser work, or in selected hair cases where the patient already has a broader plan in place. If someone has untreated hormonal loss, poor nutrition, uncontrolled inflammation, or unrealistic expectations, exosomes will not fix the larger problem.
Patients should ask direct questions before agreeing to this type of treatment. Where does the product come from? How is it processed and stored? What evidence supports this exact use? What is the regulatory status? Why is this a better fit than PRP or another established option for this patient, at this stage?
Those questions matter because access is uneven and quality varies. Some patients are paying premium pricing for a frontier therapy without a clear explanation of what problem it is supposed to solve.
For readers who want a broad public-facing overview, this anti-aging exosome therapy guide shows how the category is often presented. In practice, the job is to separate biologically plausible use from premature certainty and to place exosomes inside a larger skin, hair, recovery, or wellness strategy rather than treating them as a standalone answer.
8. Emsculpt NEO and Electromagnetic Muscle Stimulation
Emsculpt NEO belongs on this list because regenerative and restorative medicine isn't limited to skin. Body composition changes how patients age, move, and look in clothing. Muscle loss, reduced tone, and stubborn fat all affect the aesthetic picture. A tool that helps address muscle and fat non-surgically can play a real role in a complete plan.
What I like about Emsculpt NEO is that it solves a specific problem cleanly. It's useful for the patient who is already trying to live well but can't spot-train or spot-reduce their way to better contour. It's not for major weight reduction. It's for shape refinement and muscle support.
A body-composition tool, not a weight-loss replacement
This treatment makes the most sense when paired with an actual metabolic strategy. If someone has insulin resistance, hormone disruption, chronic sleep loss, or poor nutrition, body contouring alone won't carry the result. But if those systems are being addressed, device-based muscle stimulation can sharpen the outcome.
That's why it integrates well in a practice that also manages weight, hormones, and lifestyle.
- Best candidate: Patients near their goal weight who want abdominal, gluteal, arm, thigh, or calf improvement.
- Poor candidate mindset: “I don't exercise and want the device to do everything.”
- Good use case: Post-weight-loss contour support and muscle-definition enhancement without surgery.
The practical issue is maintenance. If a patient gets a nice response and then stops all exercise and nutrition discipline, the result won't hold the way they hope.
9. Hair Restoration with Low-Level Laser Therapy (LLLT) and Combination Protocols
Why do some patients use red light caps for months and still feel underwhelmed? In practice, the answer is usually diagnosis, not effort. LLLT can improve the follicular environment, but hair loss is rarely driven by one issue alone.
LLLT works by supporting cellular energy production and improving scalp conditions that favor healthier follicle function. That makes it useful for early thinning, maintenance, and post-procedure support. It does less for advanced miniaturization, active hormonal loss, scarring processes, or patients who expect a dramatic density change from light therapy alone.
The practical value of LLLT is how well it fits into a layered protocol. I use it as one part of a scalp plan that may also include PRP, targeted topicals, peptide support, and a medical review of shedding triggers such as inflammation, stress physiology, nutrient deficits, or androgen-driven loss. That integrated approach matters in aesthetic medicine because better hair outcomes often depend on fixing the biology around the follicle, not just stimulating the follicle itself.
Why combination treatment matters in hair loss
Hair restoration responds best to treatment matching. A patient with early diffuse thinning may do well with LLLT plus topical support and follow-up photography. A patient with ongoing shedding after hormonal change, metabolic strain, or long-standing pattern loss usually needs a broader plan and closer monitoring.
Consistency is the common failure point.
- What works: Regular LLLT use inside a plan that also addresses scalp health, follicle signaling, and medical contributors to hair loss.
- What falls short: Intermittent device use with no diagnosis, no tracking, and no effort to address the cause of shedding.
- When to escalate: Progressive thinning, visible miniaturization, heavy shedding, or poor response after a fair treatment window usually calls for combination therapy rather than more of the same.
Patients who want a practical breakdown of device selection, treatment expectations, and realistic use cases can review this guide to red light therapy for hair growth.
10. Hormone Optimization and Regenerative Endocrinology
What if the limiting factor in your aesthetic results is not the procedure, but the hormonal environment the procedure has to work in?
Hormone optimization is one of the most overlooked regenerative tools in an aesthetic practice. Skin quality, hair density, muscle tone, fat distribution, sleep, recovery, and inflammatory signaling are all influenced by endocrine function. When estrogen, progesterone, testosterone, thyroid hormones, cortisol patterns, or insulin regulation are off, tissue behavior changes. I see that show up as thinner skin, slower healing, increased shedding, reduced exercise recovery, and less stable body composition.
Regenerative treatments do not work in isolation; instead, they function within a biologic system. In a practice model like ProMD Health, hormone care fits into a broader strategy that connects aesthetics, metabolic health, recovery, and long-term maintenance. A patient may come in asking about skin laxity or hair loss, but the better plan sometimes starts with identifying why collagen support, follicle cycling, or muscle retention has declined in the first place.
A common example is the menopausal patient with new facial volume loss, dry skin, disrupted sleep, abdominal fat gain, and diffuse hair shedding. Filler can replace volume. Energy devices can target laxity. Hair treatments can stimulate the scalp. Those interventions may still underperform if the endocrine driver is left untreated.
The same pattern appears in men with symptomatic testosterone decline and in patients with thyroid dysfunction, insulin resistance, or chronic stress physiology.
- What hormone optimization may improve: Skin hydration and thickness, hair retention, body composition, energy, sleep quality, libido, and recovery after aesthetic procedures.
- What it requires: Proper medical history, lab evaluation, follow-up, dose adjustments, and ongoing supervision.
- What the trade-offs are: Results are not instant, dosing can need revision, and the wrong candidate or poor monitoring can create side effects instead of progress.
Patients need a clear expectation here. Hormone therapy is medical treatment with aesthetic benefits, not an aesthetic shortcut. Used well, it can improve the tissue environment so other regenerative treatments perform more predictably and hold up better over time.
That is the regenerative principle. Lasting improvement usually comes from changing the conditions that shape tissue behavior, not only treating the visible endpoint.
10-Item Regenerative Medicine Comparison
| Treatment | Implementation complexity | Resource requirements | Expected outcomes | Ideal use cases | Key advantages |
|---|---|---|---|---|---|
| Platelet-Rich Plasma (PRP) Therapy | Low–Moderate: office-based venipuncture and injection | Centrifuge, phlebotomy supplies, trained injector | Gradual collagen/hair improvement over 4–6 weeks; variable results | Hair restoration, skin texture, adjunct to microneedling | Autologous, low allergy risk, minimal downtime |
| Adipose-Derived Stem Cell Grafting (ADSCG) / SVF | High: minor surgical harvest and cell processing | Lipo-harvest equipment, cell-processing tools, surgical setting | Durable volume + progressive tissue regeneration over 6–12 months | Significant volume loss, long-term facial rejuvenation, post-bariatric restoration | Permanent/autologous volumization with biological rejuvenation |
| Biostimulatory Collagen Induction (Sculptra) | Moderate: injectable requiring reconstitution and technique | PLLA product, trained injector, multiple sessions | Progressive collagen building with 2+ years longevity; delayed visible results | Gradual facial volumization, patients preferring natural timeline | Long-lasting, stimulates native collagen, natural-looking results |
| Laser-Assisted Tissue Regeneration (Multiple Modalities) | High: modality-specific settings and risk management | Ablative/non-ablative lasers, trained operators, downtime protocols | Significant improvement in texture, scars, pigmentation; remodeling for 6–12 months | Resurfacing, scar revision, pigmentation/vascular concerns | Versatile, addresses multiple concerns; fractional options reduce downtime |
| Microneedling / Radiofrequency Microneedling | Low–Moderate: device procedure; RF adds complexity | Microneedling/RF device, sterile needles, optional PRP | Improved texture/scars over 6–12 weeks with minimal downtime | Atrophic scars, texture, pore refinement, adjunct to serums/PRP | Safe for all skin types, low downtime, cost-effective |
| Peptide Therapy & Growth Factors | Low–Moderate: prescribing and monitoring regimen | Pharmaceutical-grade peptides, reliable sourcing, follow-up testing | Systemic tissue-support effects over weeks–months; gradual benefits | Systemic regeneration, hair support, recovery optimization, longevity programs | Systemic regenerative support; complements other modalities; telehealth delivery |
| Exosome Therapy / Extracellular Vesicles | High: advanced biologics and strict handling | Characterized exosome products, -80°C storage, specialized administrators | Potent regenerative signaling; promising results but limited long-term data | Premium skin/hair rejuvenation, adjunct to microneedling/PRP for committed patients | Strong paracrine effects without cell transplant; innovation frontier |
| Emsculpt NEO (HIFEM + RF) | Low–Moderate: noninvasive device treatments in series | HIFEM+RF device, multiple sessions, contraindication screening | Measurable muscle hypertrophy and fat reduction after 4–8 sessions | Body composition improvement, post-weight-loss contouring, buttock/abdomen toning | Non-surgical dual-action (muscle + fat), minimal downtime |
| Hair Restoration with LLLT (Combination Protocols) | Low: device-based requiring consistent use | LLLT devices (home/clinic), adjunct PRP/peptides, patient compliance | Modest density gains (≈15–30%) over 3–6 months; variable responders | Androgenetic alopecia, maintenance and adjunct therapies | Safe, minimal side effects, convenient home-use for adherence |
| Hormone Optimization & Regenerative Endocrinology | High: diagnostic, individualized prescriptions and monitoring | Comprehensive lab testing, bioidentical formulations, specialist oversight | Systemic improvement in tissue quality and treatment responsiveness over weeks–months | Foundational therapy for aging, enhances outcomes across aesthetic programs | Broad systemic benefits that potentiate regenerative and aesthetic treatments |
Choosing Your Partner in Regeneration
How do you choose a regenerative medicine provider when the treatment list is long, the marketing is polished, and the real difference is in clinical judgment?
I see the same problem often. Patients assemble care from separate places, buying PRP in one office, resurfacing in another, supplements online, and hormone treatment somewhere else. The result is not always unsafe, but it is often poorly sequenced. Regenerative medicine performs best when one team sets the diagnosis, the order of treatment, the maintenance plan, and the stop points.
A strong practice should separate established therapies from emerging ones without blurring the line. PRP, collagen stimulation, laser remodeling, and RF microneedling have a clearer role in practice. Exosomes, certain peptide protocols, and other biologic add-ons may be useful in selected cases, but they require a more careful consent discussion because the evidence base is still developing. If every treatment is presented with the same level of certainty, I would question the consultation.
Range matters, but coordination matters more. Facial rejuvenation may require volume support, collagen induction, resurfacing, topical skin preparation, and endocrine review if healing or tissue quality is poor. Hair restoration may need scalp-based treatment, medical review of shedding triggers, home adherence, and follow-up photography under consistent conditions. Body composition work may include muscle stimulation, weight management, nutrition, and hormone optimization if the history supports it. The value is not in offering many services. The value is in knowing which ones belong together for a specific patient and which ones do not.
Safety is a clinical process, not a marketing claim. In regenerative care, outcomes change based on how blood products are prepared, how biologic materials are handled, where energy devices are set, how far injections are placed, and how carefully candidacy is screened. Sterility, documentation, contraindication review, and post-treatment follow-up all matter. Natural-sounding treatments still carry risk, especially when they are combined without a plan.
Cost deserves the same level of honesty. Some therapies are expensive because they require harvesting, processing, multiple visits, or specialized equipment. Others look affordable until they are repeated without a defined endpoint. I advise patients to ask a harder question than “What does this session cost?” Ask what problem the treatment is solving, how success will be measured, how many sessions are reasonable before reassessment, and what maintenance is likely.
The best regenerative programs also connect aesthetics to systemic health without forcing every patient into a wellness package. Poor recovery, diffuse hair shedding, early loss of results, persistent inflammation, and unstable body composition can reflect issues outside the treatment area. Sleep, hormones, metabolic health, nutrition, and medication review can all affect response. In an integrated practice model, those factors are assessed when they are relevant, not added automatically.
A useful consultation should end with a treatment map. What comes first, what can wait, what needs maintenance, and what is still too early or too speculative for your goals? That is the level of planning experienced patients should expect.
ProMD Health is one example of a practice structure that brings aesthetic treatments, regenerative options for skin and hair, device-based care, and medically supervised hormone, weight, and longevity services under one clinical framework. For patients who want long-term change rather than isolated procedures, that model makes practical sense.
Regeneration works best as a coordinated medical strategy. Choose the partner who can explain the trade-offs, set the sequence, and adjust the plan as your tissue response becomes clear.


