56.4% of women reported trying to lose weight within the previous year in a CDC survey, which tells you something important. The desire is there. The effort is there. For many women over 50, the problem isn't a lack of discipline. It's that the body they're working with now doesn't respond the way it did decades earlier, according to CDC weight-loss survey data.
That's why generic advice often falls flat. “Eat less and move more” sounds simple, but it ignores menopause, changing body composition, shifts in appetite signaling, medication effects, sleep disruption, and the metabolic consequences of losing muscle over time. Weight loss after 50 usually requires a different strategy, not more self-blame.
Table of Contents
- Why Weight Loss Feels Different After 50
- Understanding Your Body's New Blueprint
- Building Your Personalized Weight Loss Plan
- Comparing Commercial vs Clinical Programs
- How to Choose the Right Program for You
- The Future of Weight Management Is Integrated Care
Why Weight Loss Feels Different After 50
If your usual weight-loss strategy stopped working after 50, that does not mean you failed. It usually means your physiology changed, and the plan did not change with it.

After 50, the old playbook often stops delivering the same results because the body is working under different conditions. Menopause and the years around it can change fat distribution, sleep quality, recovery, appetite signals, and daily energy use. Age-related muscle loss can also lower calorie burn over time, especially if strength training and protein intake have been inconsistent.
That combination creates a frustrating pattern in clinic. A woman may eat about the same way she did in her 40s and still gain weight more easily. Another may add more cardio, feel more tired, and see little change in body composition. The scale can miss both problems. It does not show whether weight loss is coming from body fat, water, or muscle, and that distinction matters more in midlife.
The goal after 50 is a plan that reduces excess body fat while protecting strength, bone health, energy, and day-to-day function.
This is why medically supervised weight management deserves more attention in this age group. The useful questions are more specific than "Are you eating less?" Clinicians should look at sleep disruption, medication effects, protein intake, menopause symptoms, stress load, and whether the exercise plan is improving metabolic health or instead adding fatigue. An integrated program can connect those findings instead of treating each issue in isolation.
For a practical consumer-friendly overview of why progress can slow with age, Maximum Health Products insights on weight loss can help frame the issue in plain language. If menopause-related changes are a major part of your picture, medical options for menopause weight gain can clarify how a clinic-based approach addresses hormones, metabolism, and sustainable weight management together.
Understanding Your Body's New Blueprint

Hormones change the rules
Perimenopause and menopause don't just affect periods and hot flashes. They change the context in which weight regulation happens. As estrogen and progesterone shift, many women notice that fat accumulates more readily around the abdomen, that cravings feel different, and that recovery from poor sleep or hard workouts worsens.
This is one reason standard weight loss programs for women over 50 often miss the mark. They may mention hormones, but they rarely explain what a medically supervised program does with that information. Guidance reviewed by the Obesity Action Coalition notes that physician-supervised programs may evaluate for underlying hormonal disorders, adjust medications, or add hormone management, and that combining strength training, protein optimization, and metabolic testing can support more stable long-term outcomes, as discussed in this obesity treatment overview.
Hormones are not an excuse. They are a variable. Good care treats them that way.
Muscle becomes a metabolic asset
Muscle deserves more attention in midlife weight care. Many women have spent years focusing almost entirely on calories and cardio, yet the more important question is often whether the plan protects lean mass. If it doesn't, weight loss can become metabolically expensive. You may lose weight, but also lose strength, stability, and resting energy use.
A useful way to think about it is this. Muscle is active tissue. When it declines, the body's daily energy needs can drop. That means a plan that once worked may now be too aggressive, too restrictive, or mismatched to your current physiology.
For women who feel confused when measurements change differently from scale weight, Strive Workout's guide on body changes offers a practical explanation of why body composition matters more than scale obsession.
Practical rule: If a program talks nonstop about pounds lost but says little about muscle retention, strength, protein, or body composition, it's probably incomplete for midlife women.
Why medical supervision matters
The value of medical oversight isn't that every woman needs medication or hormone therapy. It's that midlife weight gain can have multiple drivers, and those drivers don't look the same from one patient to the next. One woman may need sleep and stress work. Another may need thyroid evaluation. Another may need medication review, strength programming, and tighter nutrition structure.
That's why a better plan starts with assessment, not assumptions. Clinicians can look at symptoms, health history, medications, menopause timing, body composition, and metabolic markers instead of forcing everyone into the same template.
If hormone-related barriers seem central to your situation, guidance on managing hormones for weight loss can help connect symptoms with a more individualized treatment path.
Building Your Personalized Weight Loss Plan
A serious plan should feel coordinated, not random. The most effective programs usually combine nutrition, resistance training, cardiovascular work, behavior change, and, when appropriate, medical support. Each part does a different job.
Nutrition that protects muscle
For women over 50, clinical guidance supports a Mediterranean-style eating pattern and a protein target of about 1.0 to 1.2 g/kg/day, or roughly 20 to 25 g per meal, with attention to calcium and vitamin D during weight loss, as outlined in this clinical nutrition overview for women over 50. That recommendation matters because weight loss shouldn't come at the cost of muscle or bone health.
In practice, that usually means meals built around:
- Protein first: fish, poultry, eggs, Greek yogurt, tofu, legumes, or other protein-rich options.
- High-fiber carbohydrates: vegetables, beans, fruit, and whole grains that improve satiety and meal quality.
- Healthy fats: olive oil, nuts, seeds, and foods that fit a Mediterranean pattern.
- Lower reliance on ultra-processed foods: not because perfection is required, but because these foods make intake harder to regulate for many people.
A common mistake is under-eating protein early in the day, then becoming overly hungry later. Another is choosing a diet that's technically low in calories but not filling, not sustainable, and not supportive of training.
Exercise that matches midlife physiology
The best exercise plan after 50 isn't the one that leaves you exhausted. It's the one you can repeat while preserving muscle, improving insulin sensitivity, and supporting cardiovascular health.
Strength training belongs at the center of that plan. It helps defend lean mass during weight loss and gives nutrition strategy somewhere productive to go. Cardio still matters, especially for endurance and heart health, but it works better as a partner to strength training than as the only tool.
For women building a home routine, simple equipment can make resistance work more approachable. MONFIT's guide to best resistance bands for seniors is a useful starting point for low-impact strength options.
A practical weekly structure often includes:
- Strength sessions: focused on major muscle groups with progressive challenge.
- Cardio work: walking, cycling, swimming, or intervals matched to fitness level and joint tolerance.
- Daily movement: steps, mobility, and non-exercise activity that keep the body from becoming sedentary between workouts.
- Recovery habits: sleep, hydration, and programming that doesn't overload an already stressed system.
If exercise leaves you hungrier, more fatigued, and less consistent, the problem may not be motivation. The dose may be wrong.
When medication and device support fit
Some women do well with lifestyle structure alone. Others need more. That doesn't mean they've failed. It means the biology is more complex.
Medical programs may consider FDA-approved anti-obesity medications, including GLP-1-based options, when a patient meets clinical criteria. These treatments can help some patients reduce intake, improve adherence, and make behavior change more achievable. They are not substitutes for protein, strength training, or follow-up. They work best inside a larger framework.
Device-based support can also have a role. Treatments such as body-contouring or muscle-stimulation technologies may help women who want an adjunct focused on body composition and muscle engagement while they continue core lifestyle treatment. These tools are not primary therapy for obesity, but they can be useful in a broader plan. One example is ProMD Health, which offers medically supervised weight management alongside options such as Emsculpt NEO within an integrated wellness setting.
Here's how the pieces fit together:
| Component | Primary Goal | Best For | Example |
|---|---|---|---|
| Nutrition planning | Create a sustainable calorie deficit while preserving lean mass | Women who have been dieting without structure or enough protein | Mediterranean-style meals with protein-forward planning |
| Strength training | Protect muscle and support metabolic rate | Women with midlife muscle loss, weakness, or body composition changes | Guided resistance sessions using weights or bands |
| Cardiovascular activity | Improve endurance, heart health, and energy expenditure | Women who tolerate aerobic exercise well | Walking, cycling, swimming, interval work |
| Behavioral support | Improve consistency and troubleshoot setbacks | Women who know what to do but struggle to maintain it | Tracking, coaching, habit review |
| Prescription treatment | Support appetite regulation and adherence when clinically appropriate | Women with persistent obesity or metabolic barriers | FDA-approved weight-loss medication under supervision |
| Device support | Complement body-composition goals | Women seeking an adjunct to exercise and nutrition | Muscle-focused or fat-reduction technology |
The trade-off is straightforward. The more personalized and medically integrated the plan is, the more coordination it requires. But that coordination is often what makes progress sustainable.
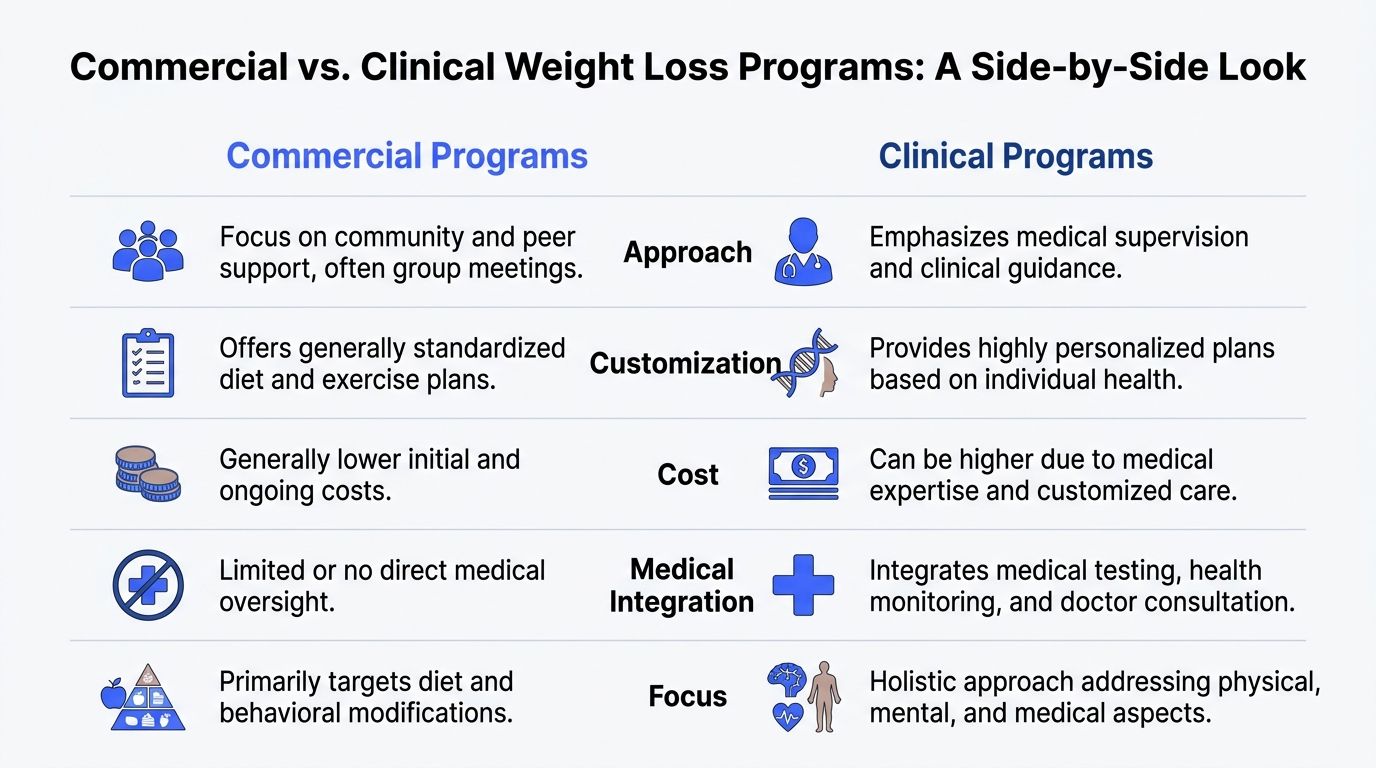
Comparing Commercial vs Clinical Programs
Commercial programs can be useful. They bring structure, accountability, meal guidance, and a system many people can follow without needing a clinic visit. For some women, that's enough to regain momentum.
Research supports that these programs can produce meaningful results. Clinical trial data reviewed in a comparative analysis found that programs such as WW, Jenny Craig, Medifast, and OPTIFAST produced average weight loss ranging from roughly 3% to 11% of baseline body weight at 12 months, and a meta-analysis of WW-based interventions found a mean loss of about 5.9 kg at one year, according to this review of commercial weight-loss programs.
Where commercial programs help
Commercial options tend to work best when the main problem is lack of structure. They can simplify food choices, encourage self-monitoring, and reduce decision fatigue.
They also tend to be more accessible. A woman who wants an organized plan, regular check-ins, and straightforward behavior tools may benefit from that format.
Still, there are limits:
- Standardization: many plans are built for broad populations, not menopause-specific physiology.
- Medical blind spots: they typically don't evaluate hormones, medication effects, or metabolic contributors.
- Body composition gaps: the scale often gets more attention than muscle retention.
Where clinical programs go further
Clinical programs become more valuable when weight gain isn't just a habits problem. If menopause symptoms, fatigue, sleep disruption, appetite changes, preexisting conditions, or medication side effects are involved, a generic system may not go far enough.
A well-run clinical program can offer:
- Medical assessment: review of symptoms, health history, medications, and relevant labs.
- Higher personalization: meal and exercise recommendations matched to body composition, tolerance, and goals.
- Prescription options: treatment pathways that commercial programs usually can't provide.
- Integrated follow-up: adjustment over time rather than a static plan.
The trade-off is cost and complexity. Clinical care often requires more appointments, more data gathering, and more active patient participation. But for women over 50 who've already tried broad commercial approaches, that extra depth is often exactly what was missing.
How to Choose the Right Program for You
The right program isn't the one with the loudest promises. It's the one that matches your biology, your medical history, and your ability to stay with the process.
Older adults can do very well in structured treatment. In the NIH-sponsored Weight-Loss Maintenance study, adults over 60 achieved stronger early results and better long-term maintenance than younger groups. During the maintenance phase, mean percent weight regain was 5.05% for those over 60, compared with higher regain in younger participants, according to the NIH-supported WLM study report. That should be reassuring. Age doesn't disqualify you from success. In a good program, it may sharpen your consistency.
Questions worth asking before you enroll
Ask direct questions. A credible clinic or program should be able to answer them clearly.
- Who evaluates me first: Will I meet with a medical professional who can assess symptoms, medications, and relevant risk factors?
- How personalized is the plan: Is the program adjusted for menopause, muscle loss, sleep issues, injuries, or metabolic concerns?
- What data do you track: Do you only track scale weight, or do you monitor body composition, symptoms, function, and adherence?
- How do you handle plateaus: Is there a process for changing nutrition, training, medication, or follow-up when progress stalls?
- What happens after the initial phase: Is there a maintenance strategy, or am I expected to figure that out myself?
A program that can't explain its maintenance plan is selling a short-term intervention, not long-term care.
Signs a program is built for long-term success
The strongest programs usually share a few characteristics.
They don't rely on extremes. They don't pretend hormones are irrelevant. They don't reduce everything to willpower. And they don't treat every woman over 50 as if she has the same needs.
Look for a program that can do the following well:
- Assess before prescribing: treatment should follow evaluation, not the other way around.
- Protect muscle while reducing fat: this is one of the most important clinical priorities after 50.
- Adjust the plan over time: the best plan at week one may not be the right plan several months later.
- Support maintenance: because losing weight and living at that new weight are different skills.
If a program gives you only food rules, it's incomplete. If it gives you only medication, it's incomplete. If it gives you only exercise, it's incomplete. Midlife weight care works better when the plan reflects the whole patient.
The Future of Weight Management Is Integrated Care
Weight management is moving away from isolated fixes. That's a good thing. Women over 50 rarely need a single intervention. They need coordinated care that treats nutrition, muscle, hormones, sleep, metabolic health, and behavior as connected issues.
One plan, not disconnected fixes
A fragmented approach creates predictable problems. One provider changes hormones without addressing nutrition. A diet plan lowers calories but ignores muscle loss. A fitness routine increases effort but doesn't account for recovery, appetite, or sleep. The patient ends up juggling conflicting advice.
Integrated care works differently. It coordinates decisions. If protein goes up, strength work should support it. If sleep is poor, recovery and hunger management need attention. If medication is added, follow-up should focus on tolerance, adherence, muscle protection, and sustainability.
This model is especially relevant now that medical options for obesity treatment have expanded. For patients exploring that route, GLP-1 medications and metabolic health are best understood as part of a broader care system, not a stand-alone answer.
Why access and follow-up change outcomes
Convenience matters more than many clinicians admit. A strong plan loses value if follow-up is hard to access. Telehealth, remote check-ins, digital tracking, and coordinated care across visits can make it easier for patients to stay engaged long enough for habits and treatment adjustments to compound.
That's the future for weight loss programs for women over 50. Not trend diets. Not punishment-based plans. Not one-size-fits-all meal charts. The better model is medically informed, muscle-conscious, menopause-aware, and flexible enough to evolve as the patient evolves.
Women over 50 aren't broken, and they're not late to the process. With the right strategy, this stage can become the point where weight management finally starts making sense.
If you want a medically supervised plan that looks at weight through the full lens of metabolism, menopause, muscle preservation, and long-term follow-up, ProMD Health offers integrated wellness care with in-person and telehealth options. The right program should help you understand your body, not fight it blindly.


