You're probably here because AOD9604 showed up the same way it does for many patients. Late-night searching. A forum thread. A clinic menu. A social post calling it a “fat-burning peptide” that sounds more precise and more advanced than standard weight loss treatment.
That starting point makes sense. People who've struggled with body composition often become very good at research. They learn enough to ask sharper questions than marketing can answer. They want to know what a compound is, what happened in real studies, whether it's safe, and why something can be discussed in wellness circles while still sitting outside standard medical practice.
AOD9604 sits right in that confusing zone. It has a real scientific origin, a plausible mechanism, and a long history of interest. It also has a major problem: what looked promising before human testing did not translate into meaningful weight loss in the trial that mattered most. That gap is the key to understanding why it never became an approved obesity drug.
If you're exploring peptide therapy, it helps to start with an evidence-based framework for medical weight management support so you can place AOD9604 in context rather than treating it like a shortcut.
Table of Contents
- Introduction A New Peptide on the Wellness Radar
- What Is AOD9604 and How Does It Work
- The Evidence Gap Preclinical Promise vs Clinical Reality
- Safety Profile and Potential Side Effects
- Legal Status and WADA Regulations
- Use in Clinical Practice and Dosing Considerations
- FAQs and How to Talk to Your Doctor
Introduction A New Peptide on the Wellness Radar
AOD9604 gets attention because it sounds like a cleaner, more targeted version of growth hormone. Many people hear that it was designed to affect fat metabolism without the broader effects of full human growth hormone, and that immediately makes it sound modern and selective.
That description is partly why the peptide keeps resurfacing. It appeals to a very specific patient mindset. Someone wants help with fat loss, but they don't want appetite suppression, don't want broad hormone exposure, and don't want to experiment blindly. AOD9604 appears to offer a middle path.
Why people get stuck on it
The online conversation usually skips the hard part. It jumps from “interesting mechanism” to “useful treatment” without spending enough time on the clinical evidence. In medicine, that leap matters.
A compound can be scientifically interesting, reasonably well tolerated, and still not be an effective treatment for the condition people want it to treat.
That's what makes the question “What is AOD9604?” more important than it sounds. The useful answer isn't just a definition. It's an honest explanation of what researchers built, what they hoped it would do, and why the results in people changed the story.
The practical issue for patients
If you're considering AOD9604, the main question isn't whether the idea is clever. It is. The main question is whether the available evidence supports using it for obesity or meaningful weight loss.
For many informed patients, that's where the confusion begins. They see it offered in some settings, they hear it described as a peptide with a favorable safety profile, and they assume there must be strong weight loss data behind it. There isn't.
What Is AOD9604 and How Does It Work
AOD9604 is a synthetic 16-amino acid peptide derived from the C-terminal fragment of human growth hormone, specifically amino acids 177 to 191. It was engineered to keep the lipolytic, or fat-breakdown, activity associated with that region of growth hormone while avoiding the broader effects linked to full-length HGH.
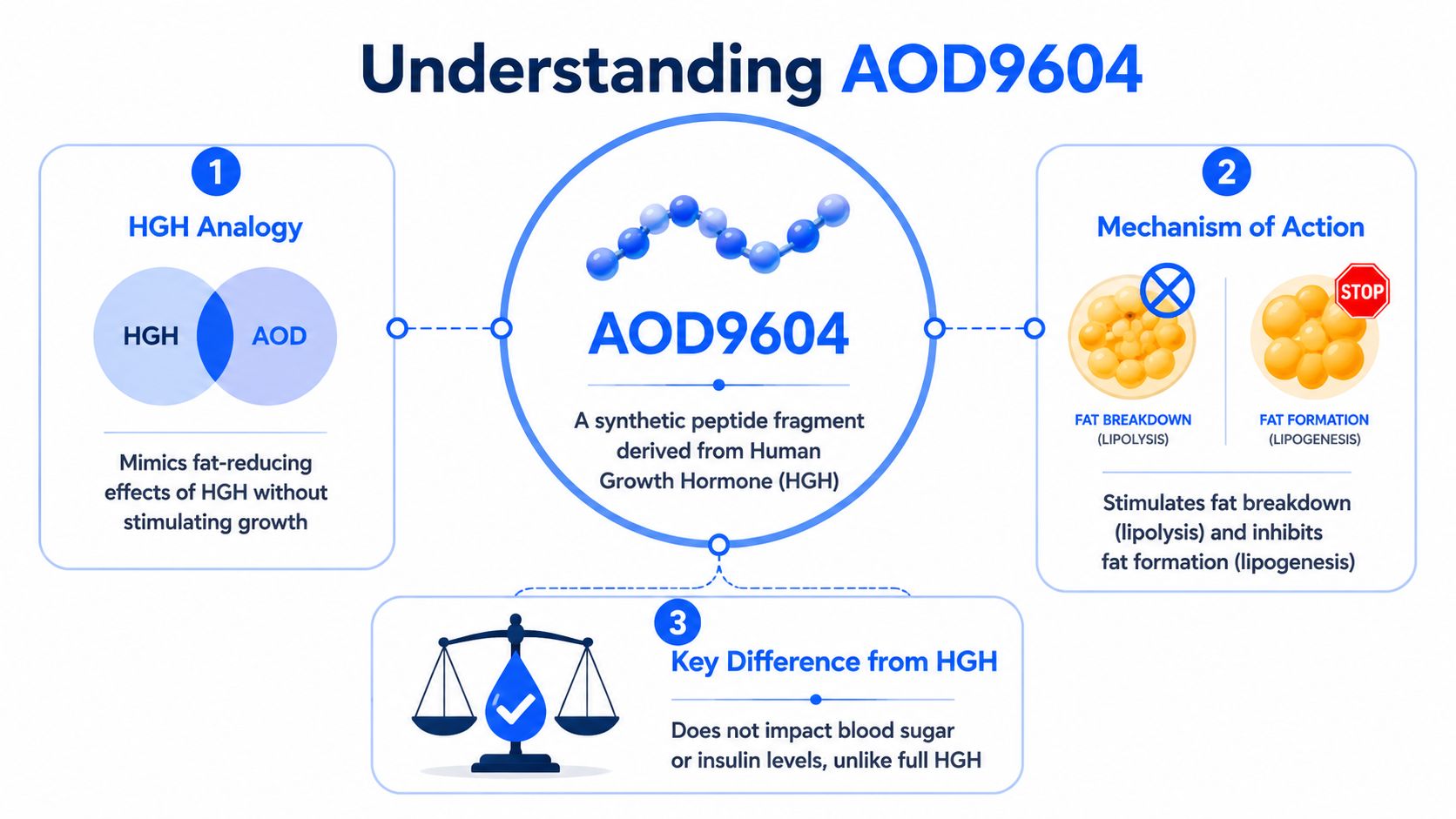
A peptide fragment, not full growth hormone
A simple way to think about it is this: full human growth hormone is like a long instruction book with many chapters. Some chapters affect growth. Some influence metabolism. Some have downstream effects that can alter glucose handling and other systems.
AOD9604 is like taking one page from the fat-metabolism chapter and trying to use only that page.
That distinction matters because many people hear “growth hormone fragment” and assume it works like HGH. It doesn't. It was specifically designed to separate one intended function from the rest of the hormone's biology.
Why researchers thought it might help with fat loss
The target was adipose tissue, or body fat. Preclinical work suggested that AOD9604 could increase lipolytic activity in fat tissue by upregulating beta-3 adrenergic receptor expression, helping restore a fat-burning response that obesity can blunt. That mechanism is one reason the peptide attracted real scientific interest rather than just internet hype.
In plain language, the idea was straightforward. If certain fat-cell signals become less responsive in obesity, maybe a selective peptide could push those signals back in the right direction.
Clinical lens: A promising mechanism is a starting point, not proof of benefit. Good obesity treatment requires meaningful human outcomes, not just elegant biology.
For readers thinking more broadly about body composition, this is also why preserving muscle during fat loss matters. A practical resource on that topic is your 2026 guide to fat loss, which explains why any fat-loss plan should be judged by more than the scale.
AOD9604 also tends to come up in discussions of peptide and regenerative care, which overlap with broader regenerative medicine applications. But in weight management, the main issue isn't theoretical fit. It's whether this targeted design produced clinically useful results in people.
The Evidence Gap Preclinical Promise vs Clinical Reality
AOD9604 becomes much easier to understand. The story has two parts, and they don't match.
Why the early data created excitement
In preclinical obese animal models, AOD9604 looked impressive. Daily oral administration of 500 microg/kg body weight for 19 days reduced body weight gain by over 50%, with 15.8 ± 0.6 g gained versus 35.6 ± 0.8 g in controls, while increasing lipolytic activity in adipose tissue according to the PubMed record describing this research.
Those kinds of findings are exactly what launch a drug-development program. The mechanism appeared coherent. The animal response appeared meaningful. The compound seemed selective in a way researchers wanted.
But animal studies answer an early question, not the final one. They tell us whether a concept deserves further testing. They do not tell us whether patients will lose clinically meaningful weight.
What happened in the human trial
The main human study was the Phase 2b OPTIONS trial. It randomized 536 obese subjects to oral AOD9604 at 0.25, 0.5, or 1 mg/day or placebo over 24 weeks. The result was the part many wellness summaries leave out: no statistically significant weight loss at any dose tested compared to placebo.
That outcome is why development for obesity treatment was terminated in 2007.
Here's the contrast at a glance:
| Metric | Preclinical (Animal) Studies | Phase 2b (Human) Trial |
|---|---|---|
| Study setting | Obese animal models | Obese human subjects |
| Dosing studied | Daily oral 500 microg/kg for 19 days | Oral 0.25, 0.5, or 1 mg/day for 24 weeks |
| Main finding | Body weight gain reduced by over 50% | No statistically significant weight loss versus placebo |
| Biological signal | Increased lipolytic activity in adipose tissue | No meaningful efficacy signal for obesity treatment |
| Development impact | Created early enthusiasm | Led to termination of obesity-drug development |
This is the central evidence gap. AOD9604 was not abandoned because it was unsafe in the way people often fear. It was abandoned because the human efficacy signal wasn't strong enough.
Why this happens in medicine
There are several reasons why a therapy can look good before human trials and then disappoint later.
- Biology is more controlled in animal models. Researchers can standardize diet, environment, and genetics more tightly than in real patients.
- Mechanism doesn't guarantee magnitude. A compound may affect a pathway without changing body weight enough to matter clinically.
- Obesity is multi-layered. Appetite, energy intake, behavior, insulin dynamics, sleep, medications, and other factors all influence outcomes.
The human trial is where a weight-loss idea has to prove it can move from biochemical plausibility to real-world clinical benefit.
That's why AOD9604 isn't an FDA-approved obesity drug. The science behind the concept was not enough. The treatment outcome in people did not meet the standard needed to justify approval and routine use for obesity.
Safety Profile and Potential Side Effects
The safety discussion around AOD9604 is more favorable than the efficacy discussion. That distinction matters because patients often assume that if a treatment failed, it must have failed because it was dangerous. In this case, the major issue was lack of convincing effectiveness for obesity treatment.

What safety looked like in trials
Historically, AOD9604 built a sizeable safety database. Across six controlled clinical trials involving over 900 participants, tolerability was described as excellent and indistinguishable from placebo. No clinically significant changes in IGF-1 were noted, and chronic treatment showed no adverse effect on insulin sensitivity and zero evidence of glucose intolerance according to the DrugBank summary of AOD9604.
That's an important difference from full-length HGH, which can impair glucose tolerance. For patients with metabolic concerns, that safety distinction is often the most medically relevant part of the AOD9604 story.
Why product quality still matters
A favorable trial safety profile doesn't mean every product sold under the name AOD9604 is automatically safe. Trial material is controlled. Real-world sourcing can be very different.
That's why any discussion of peptides should include quality control questions:
- Identity and purity: Is the compound what the label says it is?
- Compounding standards: Was it prepared by a reputable pharmacy under appropriate controls?
- Clinical oversight: Is a licensed provider monitoring response and adverse effects?
- Fit for the patient: Does the person have goals and medical conditions that make the trial history relevant at all?
If you're evaluating any wellness product or peptide source, it helps to understand how clinicians and informed consumers verify supplement purity and manufacturing standards before assuming a label reflects real quality.
AOD9604's published safety profile is reassuring. Unverified sourcing is not.
Legal Status and WADA Regulations
The legal status of AOD9604 confuses people because several different categories get blended together online. Drug approval, dietary ingredient status, compounding access, and sports regulation are not the same thing.
Not FDA approved as an obesity drug
The clearest point is this: AOD9604 does not have an FDA-approved therapeutic indication for obesity or any other condition. Its obesity-drug development was halted after the failed human efficacy program.
A separate point often gets misunderstood. The U.S. FDA granted AOD9604 Generally Recognized As Safe (GRAS) status for use as a dietary supplement ingredient in April 2026, but that is not the same as approving it as a prescription treatment. Those are different regulatory pathways with different standards and purposes.
That distinction matters because a patient may read “recognized as safe” and assume “approved to treat weight loss.” Those are not interchangeable statements.
Why athletes can't use it
People often ask a fair question: if AOD9604 didn't work well enough as an obesity drug, why is it banned in sport?
The answer is that anti-doping rules often focus on mechanism and classification, not just on whether a compound proved commercially successful. AOD9604 remains banned by the World Anti-Doping Agency under S0, Non-Approved Substances, because it is a fragment related to HGH and falls into a mechanism-based precautionary category.
So the sports ban doesn't mean AOD9604 is a powerful proven performance enhancer. It means sports regulators don't wait for that level of proof before prohibiting some hormone-related or investigational substances.
Poor clinical efficacy for obesity and anti-doping prohibition can both be true at the same time.
That kind of legal nuance comes up with many medications and controlled substances. If you want a simpler example of how people confuse approval status, scheduling, and legal classification, Fioricet's legal status explained offers a useful parallel in another area of medicine.
The practical takeaway is simple. AOD9604 is not an approved obesity drug, and competitive athletes should assume it is prohibited.
Use in Clinical Practice and Dosing Considerations
Because AOD9604 isn't a standard commercially approved obesity medication, any real-world clinical use requires more caution than many patients expect.
How it is usually accessed
In practice, compounds like this are generally discussed through the lens of compounding rather than mainstream retail dispensing. That immediately raises questions about consistency, pharmacy standards, and documentation. Those details matter more here than they do with a widely standardized approved drug.
Studies have explored both oral and subcutaneous administration. The exact doses investigated in research varied. What matters most for patients is not memorizing numbers. It's understanding that a study dose is not a personal recommendation, and a clinic protocol is not automatically evidence-based just because a peptide exists in published literature.
What a careful clinical discussion should include
If a patient wants to ask about AOD9604 responsibly, the conversation should include:
Treatment goal
Is the goal scale weight reduction, body composition refinement, or something else? AOD9604's history does not support treating it as a proven obesity medication.
Evidence threshold
How much evidence does the patient want before trying a therapy? Some people are comfortable discussing investigational or low-evidence options. Others want only treatments with established outcome data.
Source and formulation
Where would the product come from, and how is quality verified?
Monitoring plan
What symptoms, labs, and outcome measures would be followed, and when would treatment be stopped?
Better-supported alternatives
Are there approved medical options with stronger human outcome data for the patient's situation?
Some clinics, including ProMD Health's medically supervised GLP-1 and metabolic care offerings, place peptide questions inside a broader obesity-treatment discussion rather than treating a peptide as the starting point. That approach is usually more medically sound.
AOD9604 has also drawn attention in emerging cartilage repair discussions, but that's separate from the weight-management question most patients are asking when they search for it.
FAQs and How to Talk to Your Doctor

Common questions
Is AOD9604 better than GLP-1 medications for weight loss?
Not based on the human evidence discussed above. AOD9604 was designed around fat-metabolism signaling, not appetite control, and it did not show meaningful weight-loss superiority over placebo in the major obesity trial.
Why do some clinics still offer it if it isn't FDA approved?
Clinics may discuss non-approved or compounded therapies in some settings, but that doesn't mean the treatment has the same evidence level as an approved medication. The key question is whether the provider explains that distinction clearly.
Is it safe for people worried about glucose or insulin issues?
The available trial history is reassuring on that specific point, as covered earlier. Still, safety in trials doesn't replace individualized medical screening.
A simple script for your appointment
If you want a productive conversation with a qualified clinician, don't ask, “Can you prescribe this peptide?”
Ask questions like these instead:
- “I've read about AOD9604. What does the human evidence show?”
- “If it isn't FDA approved for obesity, why would someone still consider it?”
- “How does its evidence compare with approved weight-management options?”
- “If I'm focused on fat loss, what outcome should we realistically expect?”
- “How would you verify product quality and decide whether I'm a good candidate?”
“I'm not looking for hype. I want to understand the evidence, the risks, and whether a better-supported option fits my goals.”
That kind of question changes the visit. It shifts the conversation away from DIY experimentation and toward clinical reasoning.
Most patients don't need a more exotic plan. They need a clearer one.
If you want help sorting through peptide claims, obesity-treatment options, and what fits your medical history, ProMD Health offers consultations that can place AOD9604 in the proper context and review safer, better-supported pathways for weight management.