You may be in one of two places right now. You're either frustrated because you've “done everything right” with dieting and still can't keep weight off, or you're wondering whether medical weight loss is just a more expensive version of the same old cycle.
It isn't the same thing.
A core difference in medical weight loss vs dieting isn't just faster results. It's medical oversight, better tools, safer decision-making, and a plan for what happens after the scale moves. That last part's importance is often underestimated. Losing weight without a maintenance strategy often leads people right back to the same place they started, only more discouraged.
Here's the short version.
| Criterion | Medical Weight Loss | Traditional Dieting |
|---|---|---|
| Supervision | Clinician-guided with monitoring and plan adjustments | Usually self-directed |
| Main tools | Personalized nutrition, behavior support, prescription options, follow-up care | Food rules, calorie restriction, tracking apps, commercial plans |
| Expected results | Often greater weight loss in supervised programs | Often modest short-term loss |
| Safety | Ongoing review of health markers and side effects | Limited oversight |
| Long-term plan | Structured maintenance and transition support | Often stops once weight is lost |
Table of Contents
- The Cycle of Dieting and Why It Often Fails
- What Is Traditional Dieting
- What Is Medical Weight Loss
- A Side by Side Comparison of Key Differences
- The Critical Role of Long-Term Maintenance
- Who Is the Ideal Candidate for Each Approach
- How ProMD Health Crafts Your Weight Loss Journey
- Frequently Asked Questions
The Cycle of Dieting and Why It Often Fails
Dieting often fails not due to laziness, but because individuals are trying to solve a medical and behavioral problem with a rule sheet.
It usually starts the same way. Someone picks a plan, cuts out a category of food, feels highly motivated, and sees a little movement in the first few weeks. Then hunger increases, energy gets less predictable, life gets busy, and the plan becomes harder to follow than it looked on day one.
What the cycle looks like in real life
For many adults, dieting becomes a repeating loop:
- Start strong: meals are tightly controlled, snacks are removed, and motivation is high.
- Hit a plateau: the early drop slows down, even with strict effort.
- Get more restrictive: people eat less, skip meals, or eliminate more foods.
- Burn out: cravings, social fatigue, and frustration take over.
- Regain weight: old habits return because the plan was never sustainable.
That cycle is emotionally exhausting. It also teaches people the wrong lesson. They conclude that they lack discipline, when the bigger issue is that the plan didn't account for biology, stress, appetite regulation, medical history, or the need for ongoing support.
Many patients don't need more pressure. They need a framework that adapts when their body pushes back.
Why generic diets break down
Traditional dieting usually treats weight loss as a math problem alone. Eat less, move more, try harder. But that leaves out the factors that often derail progress: medication effects, sleep disruption, hormonal shifts, emotional eating patterns, muscle loss during rapid restriction, and the way hunger can intensify after weight comes off.
A structured medical program doesn't assume every stalled result is a compliance issue. It asks better questions. Is the plan too aggressive? Is appetite rising? Is muscle being lost along with fat? Are health markers changing in a way that requires adjustment?
That's why medical weight loss is distinctly different from “being on a diet.” It's designed for the point where willpower alone stops working.
What Is Traditional Dieting
Traditional dieting usually means a self-directed attempt to lose weight through food restriction, food elimination, calorie counting, fasting windows, or commercial diet rules. The person chooses the method, follows it on their own, and makes changes based on what the scale does.
That approach is common, but its long-term track record is poor. The long-term success rate for self-directed dieting has been estimated at 1% to 3% for people who lose weight and maintain that loss indefinitely, and about 45 million Americans go on a diet each year, with most regaining all lost weight within five years, according to the NCBI review on long-term outcomes of dieting.
How self-guided diets usually work
Most diets rely on one or more of the same mechanisms:
- Calorie restriction: eating less overall than the body uses.
- Macronutrient restriction: lowering carbs, fat, or both.
- Time restriction: limiting the hours when food is allowed.
- Rule-based compliance: following lists of “good” and “bad” foods.
None of these methods is automatically wrong. In some people, they create enough structure to produce initial progress. The problem is that the plan often isn't built around the individual. It's built around a philosophy.
If you work in fitness programming or want a broader look at how structured health plans are built, this guide for gym owners on program development is a useful example of how planning and accountability affect outcomes.
Why early progress often disappears
A self-directed diet often begins with enthusiasm and clear rules. That can feel productive. But without clinical oversight, people tend to interpret every short-term change as fat loss and every setback as personal failure.
Common problems show up quickly:
- Early scale drops can be misleading: some of the first change may reflect shifts in water balance rather than durable fat loss.
- Restriction becomes hard to maintain: social events, travel, stress, and fatigue all test rigid plans.
- There's no protocol for adjustment: if hunger rises or progress stalls, many people cut more food.
- Nutrition quality can suffer: self-made plans may become repetitive or imbalanced.
Traditional dieting also tends to end abruptly. People “go off” the diet, but there's no maintenance phase, no clinician review, and no strategy for what their body will do next.
What Is Medical Weight Loss
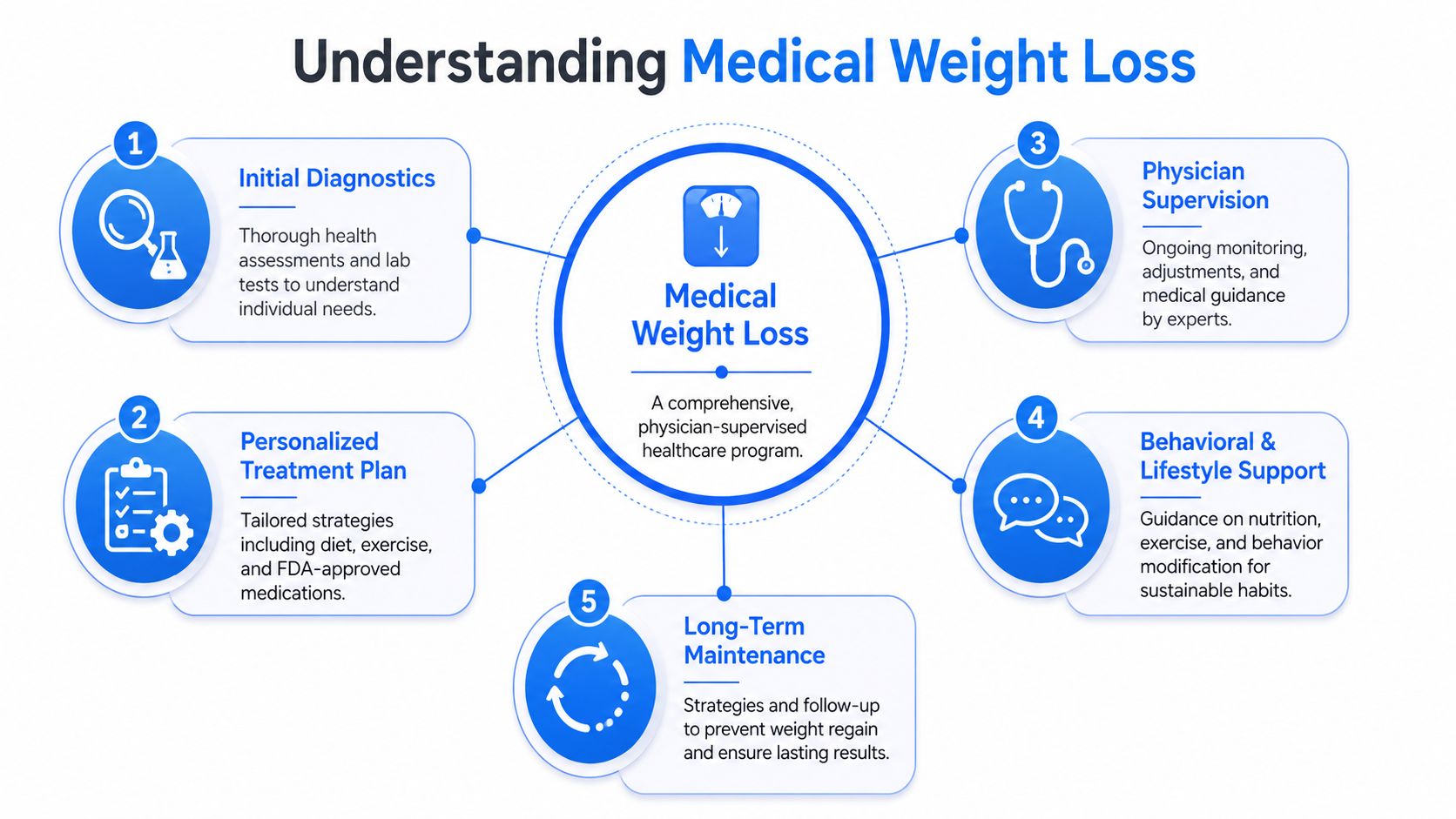
Medical weight loss is a physician-supervised healthcare program built around assessment, treatment, monitoring, and maintenance. It isn't a handout meal plan or a motivational speech about eating less. It's a clinical model for treating excess weight as a health issue with biological, behavioral, and metabolic drivers.
A clinical approach, not a generic food plan
The structure matters. A medical program starts with evaluation and then uses that information to guide treatment choices. That can include:
- Initial diagnostics: review of medical history, medications, symptoms, and relevant lab work.
- Personalized nutrition planning: guidance built around the person, not the latest trend.
- Behavioral support: identifying eating patterns, barriers, triggers, and routines that affect adherence.
- Ongoing physician supervision: follow-ups, course corrections, and safety monitoring.
Medical programs also monitor health markers during treatment. In supervised care, providers commonly follow issues such as blood pressure, HbA1c, and lipid panels while adjusting the plan as needed. That kind of ongoing support is one reason medically supervised programs report stronger adherence than self-directed efforts in the verified data provided for this topic.
For readers who want a plain-language overview of the clinical framework behind this model, the science of medical weight loss gives useful background.
Why medications change the equation for some patients
Not every patient needs medication, but modern obesity care includes tools that didn't exist in the old diet-only model. In medically supervised programs, GLP-1 receptor agonists such as semaglutide and tirzepatide have been associated with 15% to 25% total body weight loss, while lifestyle-only interventions typically yield 5% to 10%, as summarized in this medical weight loss and dieting comparison.
That doesn't mean medication replaces habit change. It means medical care can address appetite regulation and physiological barriers that make self-directed dieting so difficult for many people.
The best medical plans don't ask whether weight loss is “behavioral” or “biological.” They treat both at the same time.
A true medical weight loss program also plans beyond active loss. It protects muscle, watches for side effects, and prepares for maintenance from the beginning rather than treating maintenance as an afterthought.
A Side by Side Comparison of Key Differences
The simplest way to understand medical weight loss vs dieting is to compare what each path gives you when progress gets hard.
Medical weight loss vs traditional dieting
| Criterion | Medical Weight Loss | Traditional Dieting |
|---|---|---|
| Core model | Medical treatment plan based on individual assessment | Self-chosen food rules or commercial plan |
| Expected results | Physician-supervised programs consistently produce 2 to 3 times greater weight loss over 12 months, with 15% to 30% body weight reduction reported in supervised settings, versus about 10 pounds for standard diet-only approaches, according to Core Primary Care's review of medical weight loss outcomes | Usually modest short-term loss, often without long-term maintenance |
| Monitoring | Medical review of symptoms, side effects, and health markers | Little or no medical oversight |
| Tools available | Nutrition counseling, behavioral support, prescription therapies, follow-ups | Food restriction, tracking, self-experimentation |
| Response to plateaus | Adjust the plan based on physiology and adherence barriers | Often more restriction or abandonment |
| Maintenance strategy | Structured follow-up and transition planning | Usually unclear or absent |
| Payment model | Clinical program with direct cash-pay costs | Often lower upfront, but many people cycle through repeated attempts |
Where the real trade-offs show up
The biggest trade-off isn't convenience. It's complexity.
Traditional dieting looks simple because the instructions are simple. Cut carbs. Count calories. Skip snacks. But simplicity can become a disadvantage when the body doesn't cooperate. There's no built-in system for medication review, appetite management, muscle preservation, or adapting the plan to medical realities.
Medical care is more involved, but that's exactly why it works better for many patients. It creates structure where people usually guess.
A second trade-off is cost. Medical weight loss can involve consultation fees, follow-up visits, and medication costs. In the verified data for this topic, those costs include an initial consultation of $150 to $250, monthly follow-ups of $75 to $125, and medication costs of $300 to $550 per month without insurance, with reported downstream savings in obesity-related healthcare spending over time in some patients, based on the cited practice cost overview. ProMD Health operates on a cash-pay model, so patients should expect direct payment rather than insurance coverage.
A third trade-off is mindset. Dieting usually frames weight as a test of discipline. Medical care treats it as a chronic condition that may require several tools, including medication for the right candidate. If you want to understand how prescription support fits into a broader treatment plan, this article on GLP-1 medications and metabolic health adds helpful context.
If a patient has repeated the same self-directed cycle for years, the answer usually isn't a stricter version of the same plan.
The Critical Role of Long-Term Maintenance
Weight loss isn't finished when someone reaches a lower number on the scale. That's when the next challenge starts.
The relapse arc is real
One of the most overlooked facts in weight management is what happens after treatment changes. Emerging data shows 60% to 70% of patients regain weight within 12 months after discontinuing anti-obesity medications because physiological hunger drivers return. This pattern is often described as the relapse arc, as discussed by the Obesity Action Coalition in its treatment options overview.
That's where many consumer articles fall short. They focus on how to lose weight, but they ignore the off-ramp. If someone stops medication and has no maintenance protocol, they're often left trying to manage renewed hunger with the same willpower strategies that failed before.
What a true maintenance phase includes
A real maintenance plan isn't just “keep eating healthy.” It should include a defined transition period with support and adjustment. Clinically, that may involve:
- Medication transition planning: deciding whether to continue, taper, or stop based on response and risk.
- Lifestyle bridge support: reinforcing meal structure, movement, and behavior patterns before weight regain begins.
- Monitoring: watching appetite, symptoms, and weight trends instead of waiting for major rebound.
- Rapid intervention when needed: tightening structure early rather than after substantial regain.
Many people need more support during maintenance than they did during the first phase of loss. That's not failure. It's how chronic conditions behave.
For a deeper look at practical maintenance principles after active fat loss, the guidance on sustainable fat loss is a useful next read.
Who Is the Ideal Candidate for Each Approach
Not everyone needs the same level of intervention. The right choice depends on how much weight you need to lose, your health history, and what has or hasn't worked before.
When self-directed dieting may be reasonable
A traditional diet approach may be reasonable for someone who:
- Has a small goal: they're trying to lose a limited amount of weight rather than manage chronic obesity.
- Has no major related health concerns: there are no complicating medical issues driving weight gain or affected by it.
- Understands nutrition basics: they can build balanced meals and adjust habits without chasing extreme rules.
- Responds well to structure: they're able to stay consistent without frequent relapse.
For that person, a short-term nutrition reset or more consistent eating pattern may be enough.
When medical care is the smarter route
Medical weight loss is the more appropriate path when the issue is larger than food discipline alone. That often includes people who have dieted repeatedly, lost and regained weight multiple times, or are dealing with conditions that require safer oversight.
A clinical route is especially worth considering if:
- You've already proved dieting isn't enough: repeated cycles usually mean the model is wrong, not that you are.
- Your weight affects your health: blood sugar issues, blood pressure concerns, hormonal symptoms, or other metabolic risks raise the stakes.
- You need more than a meal plan: appetite, cravings, medication effects, and behavior patterns may all need treatment.
- You want a maintenance strategy from day one: not just a temporary push toward a goal.
There's also an access issue many people don't realize. In real-world care, anti-obesity medications are described as significantly under-prescribed, and only 2% of US patients qualifying for obesity pharmacotherapy receive it even though 50% of the population qualifies, according to the verified data tied to this underserved access discussion. For many patients, the barrier isn't willingness. It's access to appropriate medical care.
How ProMD Health Crafts Your Weight Loss Journey
The strongest weight loss programs combine clinical supervision, individualized treatment, and follow-up that continues after the early momentum phase. That's the model used in medically supervised care.
What structured care looks like in practice
A patient-centered journey usually includes an initial evaluation, review of goals and health history, a personalized plan, and regular monitoring to adjust the program over time. Depending on the individual, treatment may include prescription support, supplements, nutrition guidance, and broader wellness evaluation when hormone or lifestyle factors are affecting outcomes.
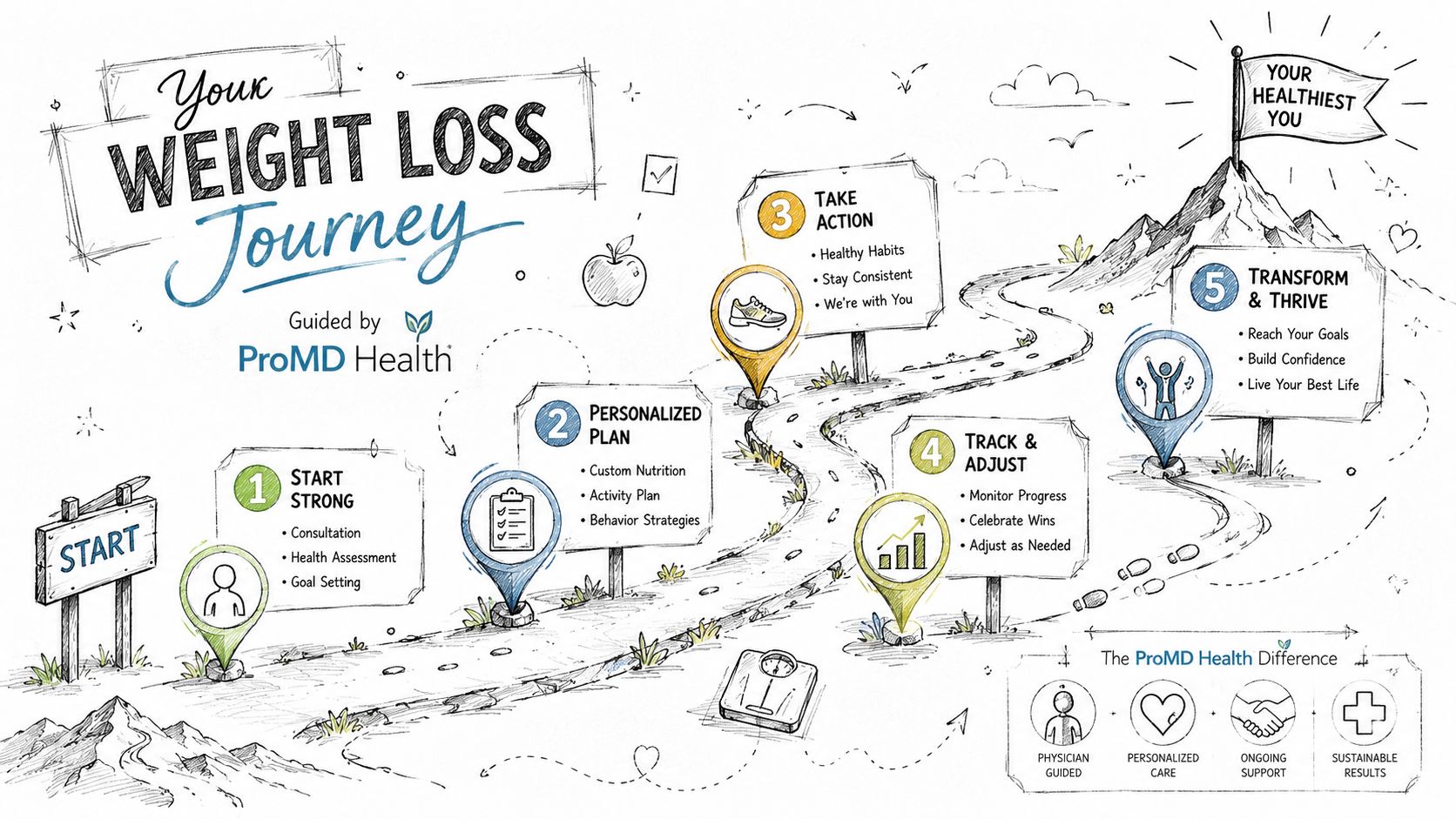
In verified data specific to this topic, medical weight loss programs at ProMD Health that combine clinical guidance, prescription medications, and supplements result in patients losing 15% to 20% of total body weight over 12 to 16 months, a greater reduction than dieting alone, according to the published ProMD Columbia location information.
Access, follow-up, and cash-pay clarity
For adults who want supervised care without relying only on in-person scheduling, medically supervised weight loss can also be accessed through the organization's broader care model, including telehealth through ProMD Connect. That matters for patients balancing work, travel, family schedules, or distance from a clinic.
ProMD Health serves approved markets including Maryland, Virginia, Washington, DC, Florida, Texas, Colorado, and Delaware. Its wellness programs are cash-pay, so patients should expect transparent direct payment rather than insurance-based coverage.
The advantage of that model is clarity. The patient knows the care plan, the follow-up structure, and the tools available from the start.
Frequently Asked Questions
Are weight loss medications like semaglutide safe?
They can be appropriate for the right patient when prescribed and monitored by a qualified clinician. Safety depends on medical history, current medications, side effects, and follow-up. That's one reason medical supervision matters.
What happens in the first consultation?
The first visit typically focuses on your health history, weight history, goals, symptoms, and treatment options. A clinician may recommend further evaluation before deciding whether nutrition changes, medication, or a broader wellness strategy makes sense.
What if I don't want to stay on medication forever?
That's an important discussion to have early. A good program includes an off-ramp strategy, not just a starting prescription. Maintenance planning should begin before weight regain starts.
How does ProMD Connect help remote patients?
It allows patients to access guided care remotely, including consultations and ongoing program management, depending on eligibility and location.
If you're tired of repeating the same diet cycle and want a structured, medically guided plan, ProMD Health offers cash-pay weight management care through in-person clinics and ProMD Connect. The next step is a consultation that looks at your health, your history, and the safest path forward for sustainable results.


